

BE-SMART (Basal Early Strategies to Maximize HbA1c Reduction with Oral Therapy): Expert Opinion
- PMID: 31102253
- PMCID: PMC6612329
- DOI: 10.1007/s13300-019-0629-z
BE-SMART (Basal Early Strategies to Maximize HbA1c Reduction with Oral Therapy): Expert Opinion
Abstract
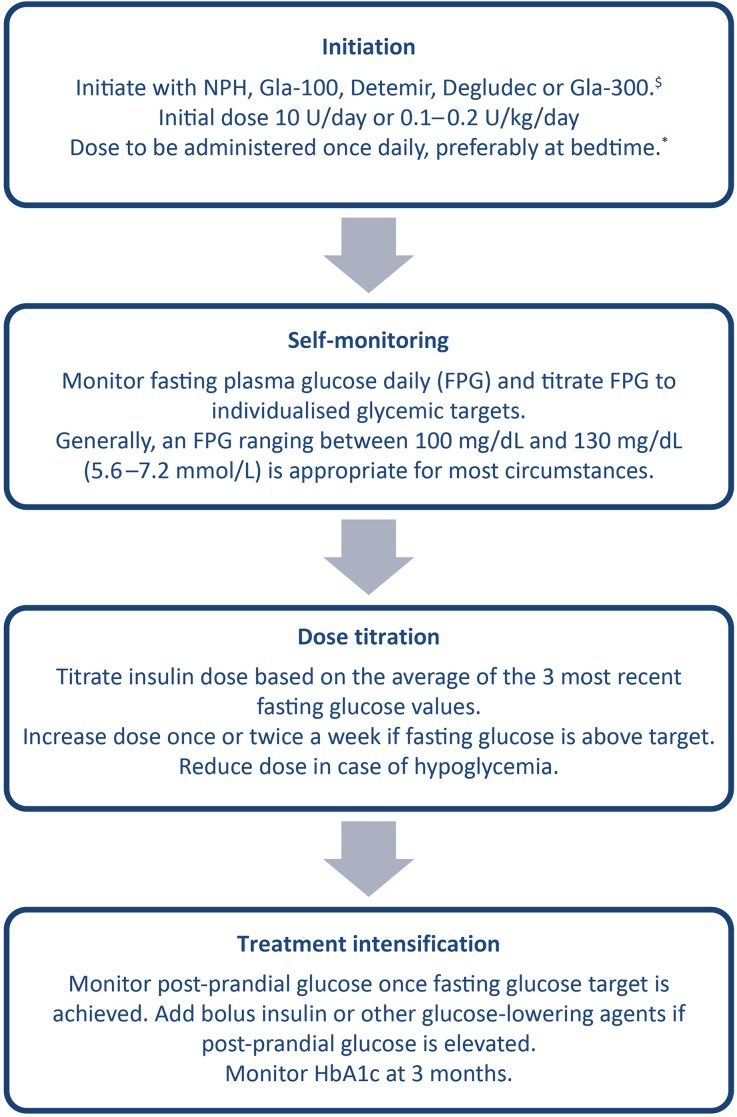
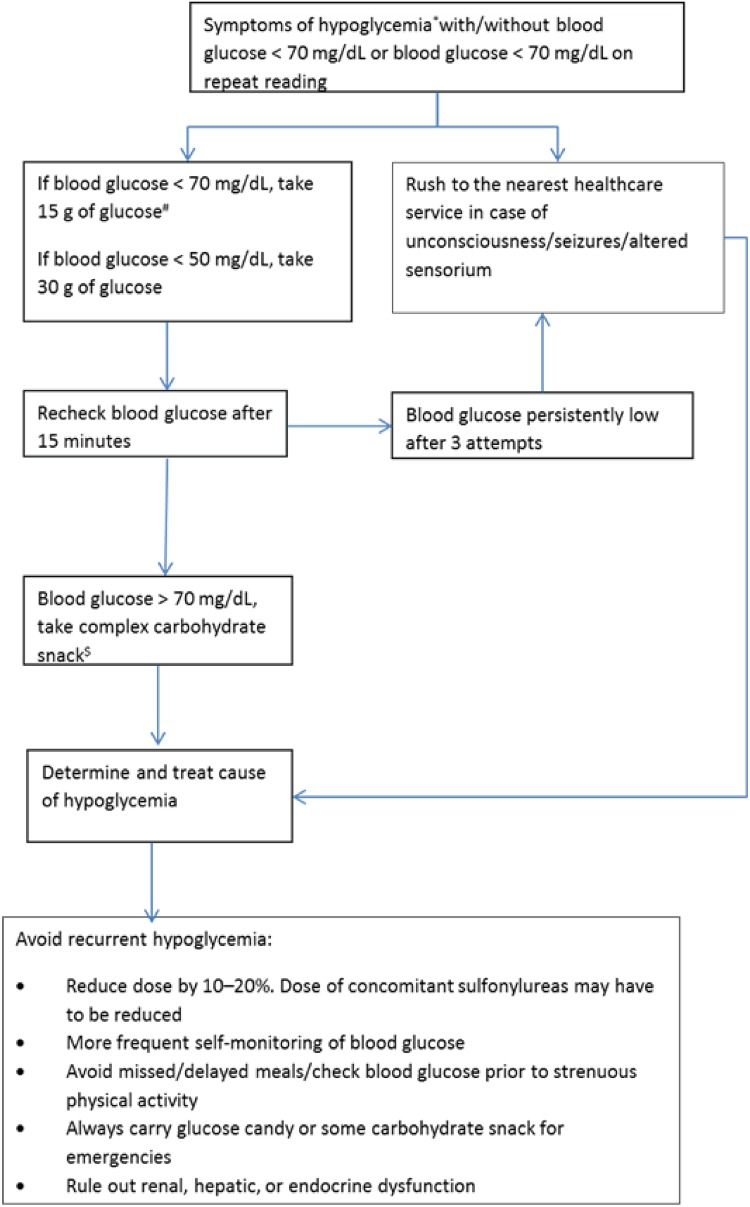
The past three decades have seen a quadruple rise in the number of people affected by diabetes mellitus worldwide, with the disease being the ninth major cause of mortality. Type 2 diabetes mellitus (T2DM) often remains undiagnosed for several years due to its asymptomatic nature during the initial stages. In India, 70% of diagnosed diabetes cases remain uncontrolled. Current guidelines endorse the initiation of insulin early in the course of the disease, specifically in patients with HbA1c > 10%, as the use of oral agents alone is unlikely to achieve glycemic targets. Early insulin initiation and optimization of glycemic control using insulin titration algorithms and patient empowerment can facilitate the effective management of uncontrolled diabetes. Early glucose control has sustained benefits in people with diabetes. However, insulin initiation, dose adjustment, and the need to repeatedly assess blood glucose levels are often perplexing for both physicians and patients, and there are misconceptions and concerns regarding its use. Hence, an early transition to insulin and ideal intensification of treatment may aid in delaying the onset of diabetes complications. This opinion statement was formulated by an expert panel on the basis of existing guidelines, clinical experience, and economic and cultural contexts. The statement stresses the timely and appropriate use of basal insulin in T2DM. It focuses on the seven vital Ts-treatment initiation, timing of administration, transportation and storage, technique of administration, targets for titration, tablets, and tools for monitoring.Funding: Sanofi.
Keywords: Basal insulin; Degludec; Detemir; Glargine; Hypoglycemia; Titration; Type 2 diabetes mellitus.
Figures
References
-
- World Health Organization. Global report on diabetes. 2016. http://apps.who.int/iris/bitstream/handle/10665/204871/9789241565257_eng.... Accessed 14 Jan 2018.
-
- International Diabetes Federation. IDF diabetes atlas. 8th ed. 2017. https://www.idf.org/e-library/epidemiology-research/diabetes-atlas.html. Accessed 15 Jan 2018.
-
- Kanungo S, Mahapatra T, Bhowmik K, et al. Diabetes scenario in a backward rural district population of India and need for restructuring of health care delivery services. Epidemiol. 2016;6(2):1. doi: 10.4172/2161-1165.1000224. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
