

Prediction of individualized lifetime benefit from cholesterol lowering, blood pressure lowering, antithrombotic therapy, and smoking cessation in apparently healthy people
- PMID: 31102402
- PMCID: PMC7229871
- DOI: 10.1093/eurheartj/ehz239
Prediction of individualized lifetime benefit from cholesterol lowering, blood pressure lowering, antithrombotic therapy, and smoking cessation in apparently healthy people
Erratum in
-
Corrigendum to: Prediction of individualized lifetime benefit from cholesterol lowering, blood pressure lowering, antithrombotic therapy, and smoking cessation in apparently healthy people.Eur Heart J. 2020 Dec 21;41(48):4579. doi: 10.1093/eurheartj/ehaa467. Eur Heart J. 2020. PMID: 32449774 Free PMC article. No abstract available.
Abstract
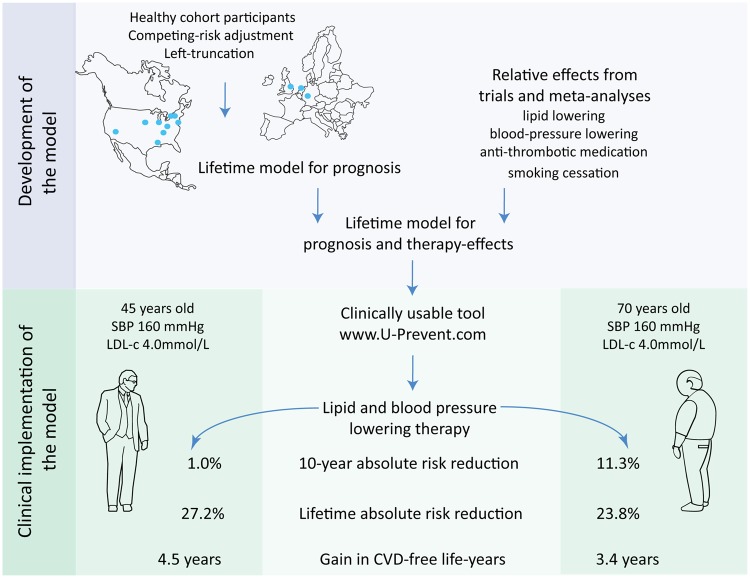
Aims: The benefit an individual can expect from preventive therapy varies based on risk-factor burden, competing risks, and treatment duration. We developed and validated the LIFEtime-perspective CardioVascular Disease (LIFE-CVD) model for the estimation of individual-level 10 years and lifetime treatment-effects of cholesterol lowering, blood pressure lowering, antithrombotic therapy, and smoking cessation in apparently healthy people.
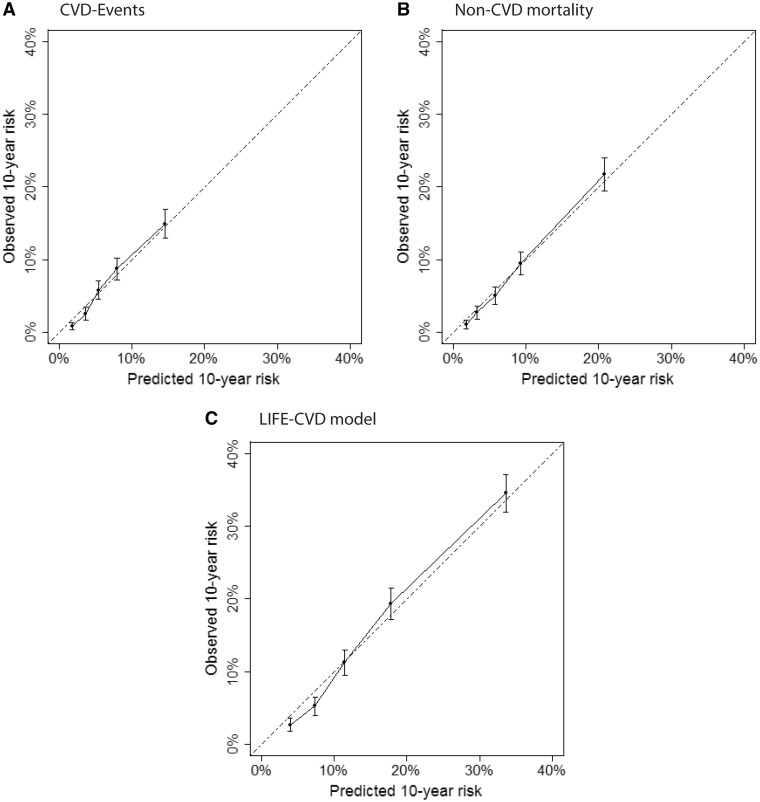
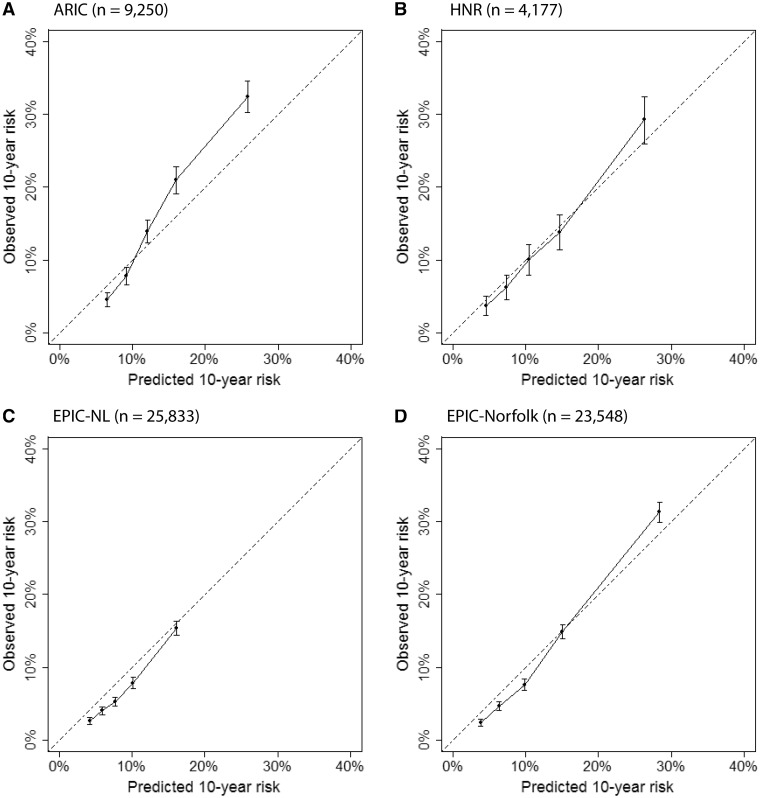
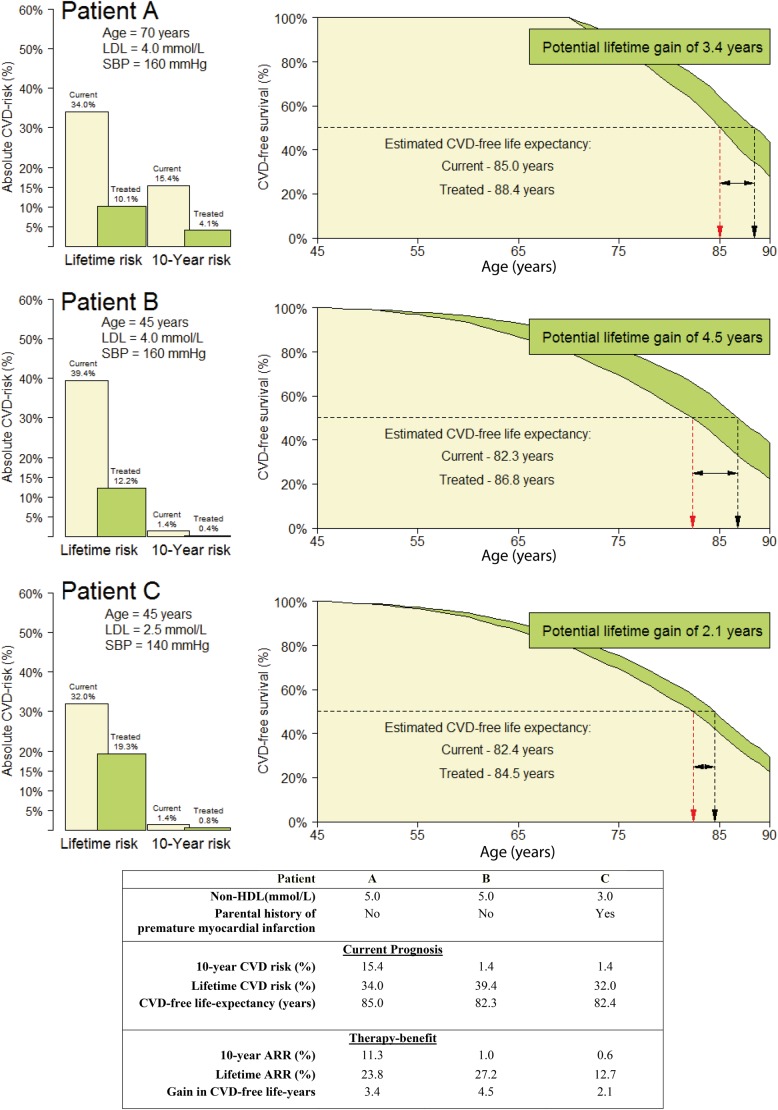
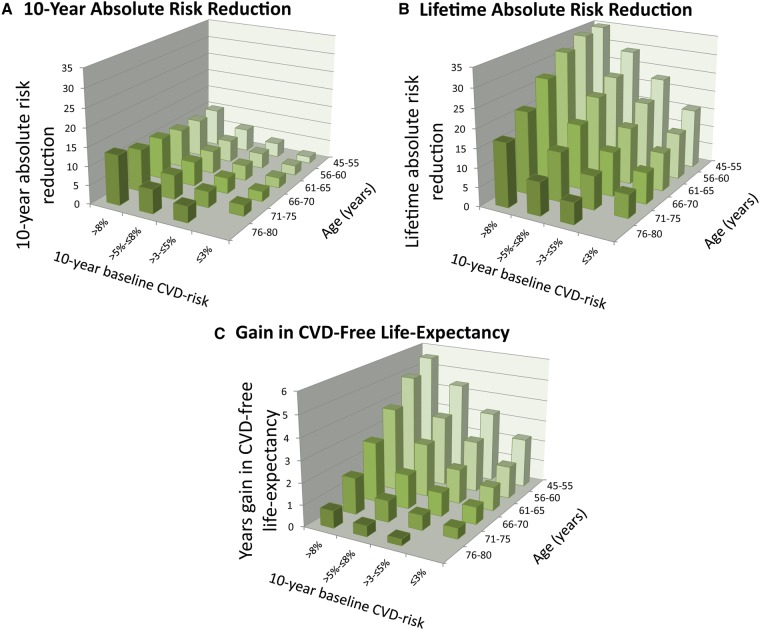
Methods and results: Model development was conducted in the Multi-Ethnic Study of Atherosclerosis (n = 6715) using clinical predictors. The model consists of two complementary Fine and Gray competing-risk adjusted left-truncated subdistribution hazard functions: one for hard cardiovascular disease (CVD)-events, and one for non-CVD mortality. Therapy-effects were estimated by combining the functions with hazard ratios from preventive therapy trials. External validation was performed in the Atherosclerosis Risk in Communities (n = 9250), Heinz Nixdorf Recall (n = 4177), and the European Prospective Investigation into Cancer and Nutrition-Netherlands (n = 25 833), and Norfolk (n = 23 548) studies. Calibration of the LIFE-CVD model was good and c-statistics were 0.67-0.76. The output enables the comparison of short-term vs. long-term therapy-benefit. In two people aged 45 and 70 with otherwise identical risk-factors, the older patient has a greater 10-year absolute risk reduction (11.3% vs. 1.0%) but a smaller gain in life-years free of CVD (3.4 vs. 4.5 years) from the same therapy. The model was developed into an interactive online calculator available via www.U-Prevent.com.
Conclusion: The model can accurately estimate individual-level prognosis and treatment-effects in terms of improved 10-year risk, lifetime risk, and life-expectancy free of CVD. The model is easily accessible and can be used to facilitate personalized-medicine and doctor-patient communication.
Keywords: Apparently healthy people; Cardiovascular disease prevention; Lifetime prediction; Therapy-benefit.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2019. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Prediction of individualized lifetime benefit from cardiovascular risk-reducing interventions in apparently healthy people.Eur Heart J. 2020 Mar 14;41(11):1200-1202. doi: 10.1093/eurheartj/ehz515. Eur Heart J. 2020. PMID: 31369081 No abstract available.
References
-
- Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, Hoes AW, Jennings CS, Landmesser U, Pedersen TR, Reiner Z, Riccardi G, Taskinen MR, Tokgozoglu L, Monique Verschuren WM, Vlachopoulos C, Wood DA, Luis Zamorano J, Additional C, Cooney MT.. 2016 ESC/EAS guidelines for the management of dyslipidaemias. Rev Esp Cardiol (Engl Ed) 2017;70:115.. - PubMed
-
- Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, Braun LT, de Ferranti S, Faiella-Tommasino J, Forman DE, Goldberg R, Heidenreich PA, Hlatky MA, Jones DW, Lloyd-Jones D, Lopez-Pajares N, Ndumele CE, Orringer CE, Peralta CA, Saseen JJ, Smith SC Jr, Sperling L, Virani SS, Yeboah J.. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2018.
-
- Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, Smith SC Jr, Spencer CC, Stafford RS, Taler SJ, Thomas RJ, Williams KA Sr, Williamson JD, Wright JT Jr. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2018;138:e484–e594. - PubMed
-
- Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, Clement DL, Coca A, de Simone G, Dominiczak A, Kahan T, Mahfoud F, Redon J, Ruilope L, Zanchetti A, Kerins M, Kjeldsen SE, Kreutz R, Laurent S, Lip GYH, McManus R, Narkiewicz K, Ruschitzka F, Schmieder RE, Shlyakhto E, Tsioufis C, Aboyans V, Desormais I; ESC Scientific Document Group. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J 2018;39:3021–3104. - PubMed
-
- Goff DC Jr, Lloyd-Jones DM, Bennett G, Coady S, D'Agostino RB, Gibbons R, Greenland P, Lackland DT, Levy D, O'Donnell CJ, Robinson JG, Schwartz JS, Shero ST, Smith SC Jr, Sorlie P, Stone NJ, Wilson PW, Jordan HS, Nevo L, Wnek J, Anderson JL, Halperin JL, Albert NM, Bozkurt B, Brindis RG, Curtis LH, DeMets D, Hochman JS, Kovacs RJ, Ohman EM, Pressler SJ, Sellke FW, Shen WK, Smith SC Jr, Tomaselli GF; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014;129:S49–S73. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- MC_UU_12015/1/MRC_/Medical Research Council/United Kingdom
- HHSN268201700002C/HL/NHLBI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- HHSN268201700003I/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- MR/N003284/1/MRC_/Medical Research Council/United Kingdom
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- G1000143/MRC_/Medical Research Council/United Kingdom
- N01 HC095167/HL/NHLBI NIH HHS/United States
- HHSN268201700001I/HL/NHLBI NIH HHS/United States
- 14136/CRUK_/Cancer Research UK/United Kingdom
- G0401527/MRC_/Medical Research Council/United Kingdom
- HHSN268201700004I/HL/NHLBI NIH HHS/United States
- HHSN268201700005C/HL/NHLBI NIH HHS/United States
- HHSN268201700001C/HL/NHLBI NIH HHS/United States
- HHSN268201700003C/HL/NHLBI NIH HHS/United States
- HHSN268201700004C/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- HHSN268201700002I/HL/NHLBI NIH HHS/United States
- HHSN268201700005I/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
