

Varied influence of the femoral or tibial component on quadriceps angles: Verified by imaging studies
- PMID: 31103418
- PMCID: PMC6738274
- DOI: 10.1016/j.aott.2019.04.011
Varied influence of the femoral or tibial component on quadriceps angles: Verified by imaging studies
Abstract
Objective: The aim of this study was to evaluate the varied influence of femoral or tibial component on Quadriceps angles (Q-angle) measured with magnetic resonance image (MRI) and full-length standing scanogram (FLSS) techniques.
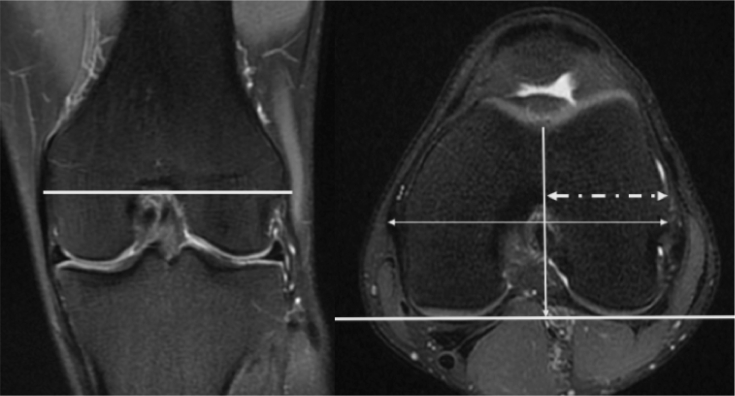
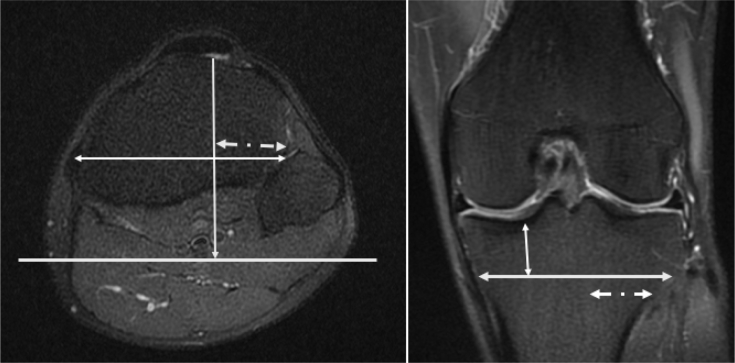
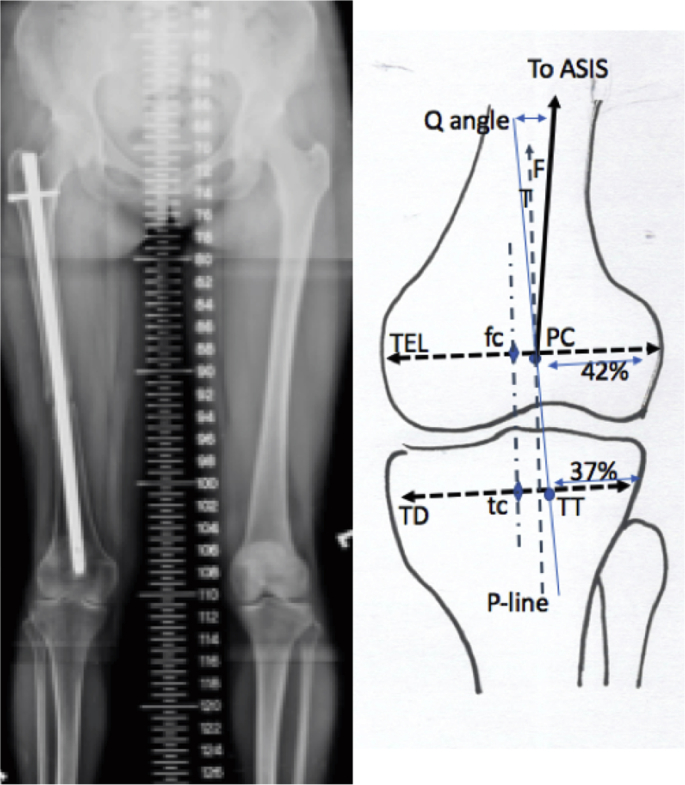
Methods: Two groups of patients were studied. The first group underwent MRI studies and the second group underwent FLSS studies. Two-step procedures were carried out. Knee MRI in 60 consecutive adult patients simply taken for meniscus or ligament injuries were utilized at the first step. The standardized patellar center (PC) and tibial tubercle (TT) on the frontal plane of MRI were positioned. At the second step, the FLSS in other 100 consecutive young adult patients taken for chronic unilateral lower extremity injuries were used for locating the two landmarks from MRI. The Q-angle was then determined on the anterior superior iliac spine, standardized PC, and TT on the FLSS.
Results: For 60 patients, the standardized PC was at the point 42% from the lateral end of the trans-epicondylar line of the femur. The TT was at the point 2 cm distal to the tibial articular surface and 37% from the lateral end of the tibial width. For 100 patients, the Q-angle was an average of 9.5° and 65.2% of the Q-angle was contributed by the upper arm (the femur). Women had a larger Q-angle (10.1° vs. 8.8°, p = 0.02) and a shorter femur (41.1 vs. 44.7 cm, p < 0.001).
Conclusion: The Q-angle is about 9.5° with 65.2% contributed by the femur. The Q-angle may mainly be influenced by the femoral component.
Level of evidence: Level IV, Diagnostic Study.
Keywords: Femoral component; Full-length standing scanogram; Influence; Magnetic resonance images; Quadriceps angle; Tibial component.
Copyright © 2019 Turkish Association of Orthopaedics and Traumatology. Production and hosting by Elsevier B.V. All rights reserved.
Figures
Similar articles
-
Radiological Verification for the Suitability of Using the Quadriceps Angle to Represent Orientation of the Quadriceps Femoris.Orthop Surg. 2024 Jul;16(7):1726-1731. doi: 10.1111/os.14093. Epub 2024 May 20. Orthop Surg. 2024. PMID: 38766778 Free PMC article.
-
Imaging Approaches for Accurate Determination of the Quadriceps Angle.Orthop Surg. 2020 Aug;12(4):1270-1276. doi: 10.1111/os.12708. Epub 2020 Jun 16. Orthop Surg. 2020. PMID: 32548902 Free PMC article.
-
Defining the Role of the Tibial Tubercle-Trochlear Groove and Tibial Tubercle-Posterior Cruciate Ligament Distances in the Work-up of Patients With Patellofemoral Disorders.Am J Sports Med. 2015 Jun;43(6):1348-53. doi: 10.1177/0363546515576128. Epub 2015 Mar 26. Am J Sports Med. 2015. PMID: 25813867
-
Variations in Knee Kinematics After ACL Injury and After Reconstruction Are Correlated With Bone Shape Differences.Clin Orthop Relat Res. 2017 Oct;475(10):2427-2435. doi: 10.1007/s11999-017-5368-8. Clin Orthop Relat Res. 2017. PMID: 28451863 Free PMC article.
-
A Systematic Review on Quadriceps Angle in Relation to Knee Abnormalities.Cureus. 2023 Jan 29;15(1):e34355. doi: 10.7759/cureus.34355. eCollection 2023 Jan. Cureus. 2023. PMID: 36874732 Free PMC article. Review.
Cited by
-
Radiological Verification for the Suitability of Using the Quadriceps Angle to Represent Orientation of the Quadriceps Femoris.Orthop Surg. 2024 Jul;16(7):1726-1731. doi: 10.1111/os.14093. Epub 2024 May 20. Orthop Surg. 2024. PMID: 38766778 Free PMC article.
-
Can isokinetic test be a supportive tool for unilateral knee arthroplasty decision?Turk J Phys Med Rehabil. 2023 Feb 28;69(1):105-110. doi: 10.5606/tftrd.2023.12374. eCollection 2023 Mar. Turk J Phys Med Rehabil. 2023. PMID: 37201003 Free PMC article.
References
-
- Lankhorst N.E., Bierma-Zeinstra S.M., van Middelkoop M. Factors associated with patellofemoral pain syndrome: a systemic review. Br J Sport Med. 2013;47:193–206. - PubMed
-
- Brattstroem H. Shape of the intercondylar groove normally and in recurrent dislocation of patella. A clinical and X-ray-anatomical investigation. Acta Orthop Scand. 1964;68:S1–S148. - PubMed
-
- Park S.K., Stefanyshyn D.J. Greater Q angle may not be a risk factor of patellofemoral pain syndrome. Clin Biomech. 2011;26:392–396. - PubMed
-
- Grelsamer R.P., Dubey A., Weinstein C.H. Men and women have similar Q angles: a clinical and trigonometric evaluation. J Bone Joint Surg Br. 2005;87:1498–1501. - PubMed
-
- Smith T.O., Hunt N.J., Donell S.T. The reliability and validity of the Q-angle: a systemic review. Knee Surg Sport Traumatol Arthrosc. 2008;16:1068–1079. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
