

Mild Cognitive Impairment and Decline in Resting State Functional Connectivity after Total Knee Arthroplasty with General Anesthesia
- PMID: 31104019
- PMCID: PMC6629260
- DOI: 10.3233/JAD-180932
Mild Cognitive Impairment and Decline in Resting State Functional Connectivity after Total Knee Arthroplasty with General Anesthesia
Abstract
Background: Research shows that older adults can have a decline in three key resting state networks (default mode network, central executive network, and salience network) after total knee arthroplasty and that patients' pre-surgery brain and cognitive integrity predicts decline.
Objectives: First, to assess resting state network connectivity decline from the perspective of nodal connectivity changes in a larger older adult surgery sample. Second, to compare pre-post functional connectivity changes in mild cognitive impairment (MCI) versus non-MCI.
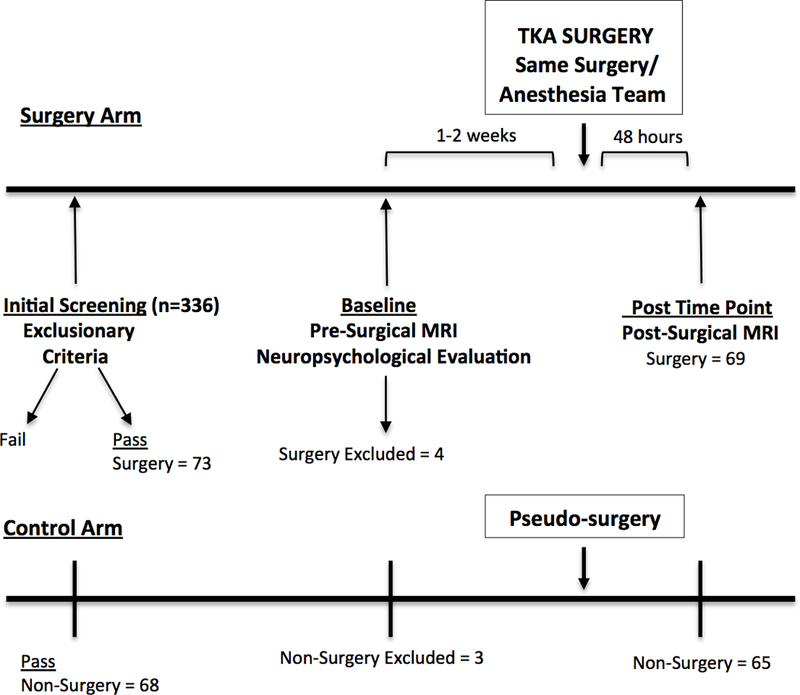
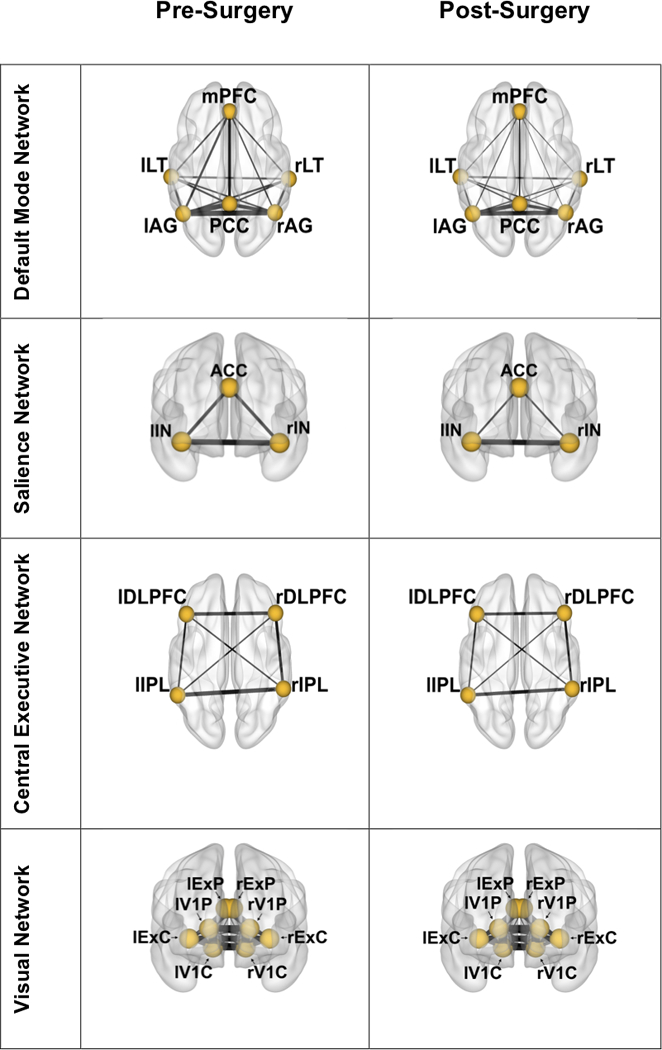
Methods: Surgery (n = 69) and non-surgery (n = 65) peers completed a comprehensive preoperative neuropsychological evaluation and pre- and acute (within 48 hours) post-surgery/pseudo-surgery functional brain magnetic resonance imaging scan. MCI was classified within both (MCI surgery, n = 13; MCI non-surgery, n = 10). Using standard coordinates, we defined default mode network, salience network, central executive network, and the visual network (serving as a control network). The functional connectivity of these networks and brain areas (nodes) that make up these networks were examined for pre-post-surgery changes through paired samples t-test and ANOVA.
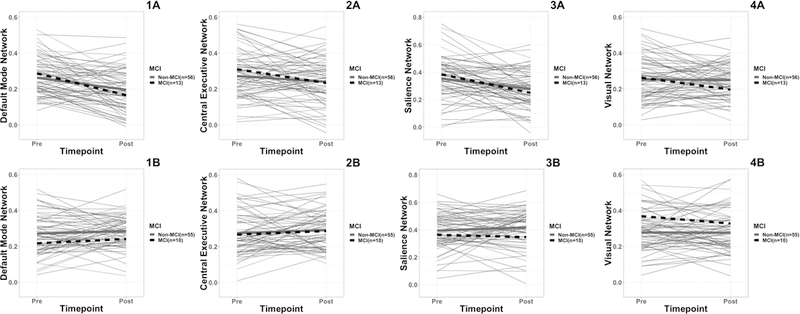
Results: There was a decline in RSN connectivity after surgery (p < 0.05) only in the three cognitive networks (not the visual network). The default mode and salience network showed nodal connectivity changes (p < 0.01). MCI surgery had greater functional connectivity decline in DMN and SN. Non-surgery participants showed no significant functional connectivity change.
Conclusion: Surgery with general anesthesia selectively alters functional connectivity in major cognitive resting state networks particularly in DMN and SN. Participants with MCI appear more vulnerable to these functional changes.
Keywords: Anesthesia; cognitive dysfunction; dementia; functional magnetic resonance imaging; mild cognitive impairment; orthopedics; surgery.
Conflict of interest statement
The authors have no conflict of interest to report.
Figures
References
-
- Abildstrom H, Rasmussen LS, Rentowl P, Hanning CD, Rasmussen H, Kristensen PA, Moller JT (2000) Cognitive dysfunction 1–2 years after non-cardiac surgery in the elderly Acta Anesthesiologia Scandanavia 44, 1246–1251. - PubMed
-
- Rasmussen LS, Johnson T, Kuipers HM, Kristensen D, Siersma VD, Vila P, Jolles J, Papaioannou A, Abildstrom H, Silverstein JH, Bonal JA, Raeder J, Nielsen IK, Kortilla K, Munoz L, Dodds C, Hanning CD, Moller JT (2003) Does anaesthesia cause postoperative cognitive dysfunction? A randomised study of regional versus general anaesthesia in 438 elderly patients. Acta Anaesthesiologica Scandinavica 47, 260–266. - PubMed
-
- Xie G, Deschamps A, Backman SB, Fiset P, Chartrand D, Dagher A, Plourde G (2011) Critical involvement of the thalamus and precuneus during restoration of consciousness with physostigmine in humans during propofol anaesthesia: a positron emission tomography study. Br J Anaesth 106, 548–557. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
