

Burosumab versus conventional therapy in children with X-linked hypophosphataemia: a randomised, active-controlled, open-label, phase 3 trial
- PMID: 31104833
- PMCID: PMC7179969
- DOI: 10.1016/S0140-6736(19)30654-3
Burosumab versus conventional therapy in children with X-linked hypophosphataemia: a randomised, active-controlled, open-label, phase 3 trial
Erratum in
-
Department of Error.Lancet. 2019 Jul 13;394(10193):120. doi: 10.1016/S0140-6736(19)31426-6. Epub 2019 Jul 11. Lancet. 2019. PMID: 31305251 No abstract available.
Abstract
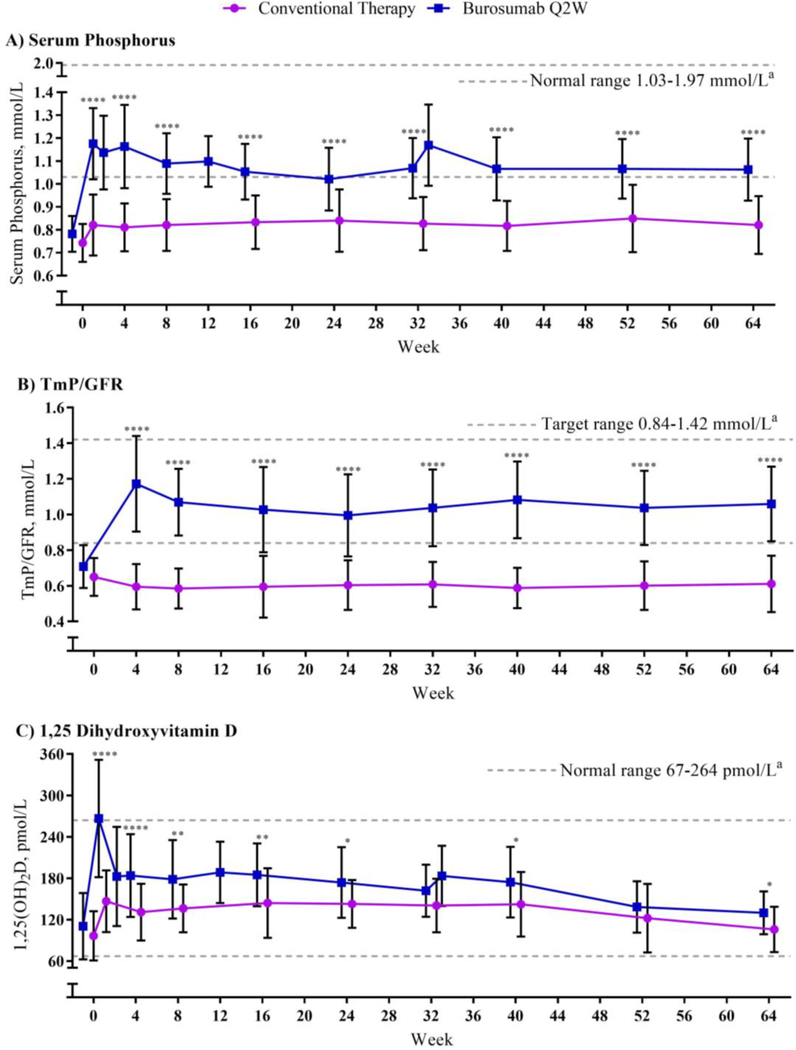
Background: X-linked hypophosphataemia in children is characterised by elevated serum concentrations of fibroblast growth factor 23 (FGF23), hypophosphataemia, rickets, lower extremity bowing, and growth impairment. We compared the efficacy and safety of continuing conventional therapy, consisting of oral phosphate and active vitamin D, versus switching to burosumab, a fully human monoclonal antibody against FGF23, in paediatric X-linked hypophosphataemia.
Methods: In this randomised, active-controlled, open-label, phase 3 trial at 16 clinical sites, we enrolled children with X-linked hypophosphataemia aged 1-12 years. Key eligibility criteria were a total Thacher rickets severity score of at least 2·0, fasting serum phosphorus lower than 0·97 mmol/L (3·0 mg/dL), confirmed PHEX (phosphate-regulating endopeptidase homolog, X-linked) mutation or variant of unknown significance in the patient or a family member with appropriate X-linked dominant inheritance, and receipt of conventional therapy for at least 6 consecutive months for children younger than 3 years or at least 12 consecutive months for children older than 3 years. Eligible patients were randomly assigned (1:1) to receive either subcutaneous burosumab starting at 0·8 mg/kg every 2 weeks (burosumab group) or conventional therapy prescribed by investigators (conventional therapy group). Both interventions lasted 64 weeks. The primary endpoint was change in rickets severity at week 40, assessed by the Radiographic Global Impression of Change global score. All patients who received at least one dose of treatment were included in the primary and safety analyses. The trial is registered with ClinicalTrials.gov, number NCT02915705.
Findings: Recruitment took place between Aug 3, 2016, and May 8, 2017. Of 122 patients assessed, 61 were enrolled. Of these, 32 (18 girls, 14 boys) were randomly assigned to continue receiving conventional therapy and 29 (16 girls, 13 boys) to receive burosumab. For the primary endpoint at week 40, patients in the burosumab group had significantly greater improvement in Radiographic Global Impression of Change global score than did patients in the conventional therapy group (least squares mean +1·9 [SE 0·1] with burosumab vs +0·8 [0·1] with conventional therapy; difference 1·1, 95% CI 0·8-1·5; p<0·0001). Treatment-emergent adverse events considered possibly, probably, or definitely related to treatment by the investigator occurred more frequently with burosumab (17 [59%] of 29 patients in the burosumab group vs seven [22%] of 32 patients in the conventional therapy group). Three serious adverse events occurred in each group, all considered unrelated to treatment and resolved.
Interpretation: Significantly greater clinical improvements were shown in rickets severity, growth, and biochemistries among children with X-linked hypophosphataemia treated with burosumab compared with those continuing conventional therapy.
Funding: Ultragenyx Pharmaceutical and Kyowa Kirin International.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Figures



Comment in
-
Burosumab treatment of children with X-linked hypophosphataemic rickets.Lancet. 2019 Jun 15;393(10189):2364-2366. doi: 10.1016/S0140-6736(19)31054-2. Epub 2019 May 16. Lancet. 2019. PMID: 31104830 No abstract available.
References
-
- Carpenter TO, Shaw NJ, Portale AA, Ward LM, Abrams SA, Pettifor JM. Rickets. Nat Rev Dis Primers. 2017; 3: 17101. - PubMed
-
- Glorieux FH, Marie PJ, Pettifor JM, Delvin EE. Bone response to phosphate salts, ergocalciferol, and calcitriol in hypophosphatemic vitamin D-resistant rickets. N Engl J Med. 1980; 303(18): 1023–31. - PubMed
-
- West CD, Blanton JC, Silverman FN, Holland NH. Use of phosphate salts as an adjunct to vitamin D in the treatment of hypophosphatemic vitamin D refractory rickets. J Pediatr. 1964; 64(4): 469–77. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
