

Optimizing Epicardial Restraint and Reinforcement Following Myocardial Infarction: Moving Towards Localized, Biomimetic, and Multitherapeutic Options
- PMID: 31105193
- PMCID: PMC6477619
- DOI: 10.3390/biomimetics4010007
Optimizing Epicardial Restraint and Reinforcement Following Myocardial Infarction: Moving Towards Localized, Biomimetic, and Multitherapeutic Options
Abstract
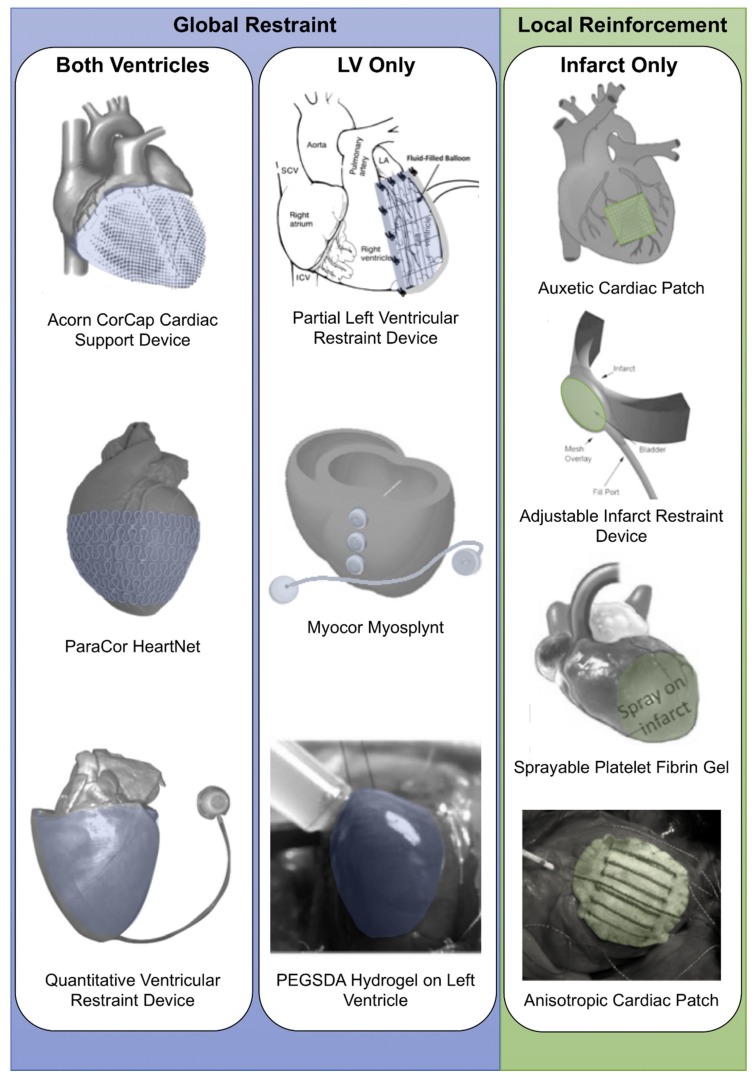
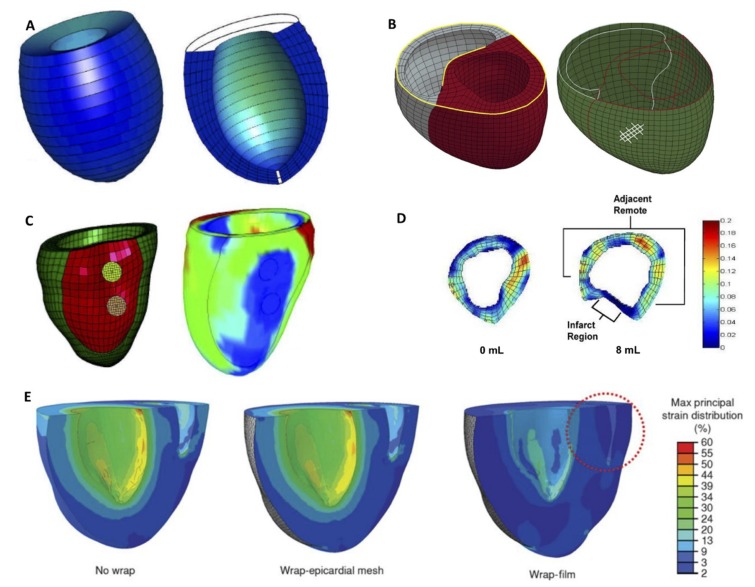
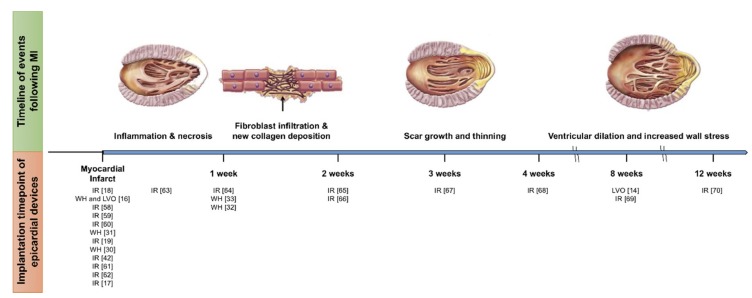
The mechanical reinforcement of the ventricular wall after a myocardial infarction has been shown to modulate and attenuate negative remodeling that can lead to heart failure. Strategies include wraps, meshes, cardiac patches, or fluid-filled bladders. Here, we review the literature describing these strategies in the two broad categories of global restraint and local reinforcement. We further subdivide the global restraint category into biventricular and univentricular support. We discuss efforts to optimize devices in each of these categories, particularly in the last five years. These include adding functionality, biomimicry, and adjustability. We also discuss computational models of these strategies, and how they can be used to predict the reduction of stresses in the heart muscle wall. We discuss the range of timing of intervention that has been reported. Finally, we give a perspective on how novel fabrication technologies, imaging techniques, and computational models could potentially enhance these therapeutic strategies.
Keywords: biomimetics; infarct reinforcement; ventricular restraint.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Ventricular restraint prevents infarct expansion and improves borderzone function after myocardial infarction: a study using magnetic resonance imaging, three-dimensional surface modeling, and myocardial tagging.Ann Thorac Surg. 2007 Dec;84(6):2004-10. doi: 10.1016/j.athoracsur.2007.06.062. Ann Thorac Surg. 2007. PMID: 18036925
-
Infarct size reduction and attenuation of global left ventricular remodeling with the CorCap cardiac support device following acute myocardial infarction in sheep.Heart Fail Rev. 2005 Jun;10(2):125-39. doi: 10.1007/s10741-005-4640-2. Heart Fail Rev. 2005. PMID: 16258720
-
Delivery of cardiovascular progenitors with biomimetic microcarriers reduces adverse ventricular remodeling in a rat model of chronic myocardial infarction.Acta Biomater. 2021 May;126:394-407. doi: 10.1016/j.actbio.2021.03.017. Epub 2021 Mar 11. Acta Biomater. 2021. PMID: 33716175
-
Modulation of left ventricular dilation remodeling with epicardial restraint devices in postmyocardial infarction heart failure.Curr Heart Fail Rep. 2009 Dec;6(4):229-35. doi: 10.1007/s11897-009-0032-6. Curr Heart Fail Rep. 2009. PMID: 19948091 Review.
-
The reduction of infarct size--forty years of research.Rev Port Cardiol. 2010 Jun;29(6):1037-53. Rev Port Cardiol. 2010. PMID: 20964114 Review. English, Portuguese.
Cited by
-
Utilization of Engineering Advances for Detailed Biomechanical Characterization of the Mitral-Ventricular Relationship to Optimize Repair Strategies: A Comprehensive Review.Bioengineering (Basel). 2023 May 17;10(5):601. doi: 10.3390/bioengineering10050601. Bioengineering (Basel). 2023. PMID: 37237671 Free PMC article. Review.
-
Sequential delivery of cardioactive drugs via microcapped microneedle patches for improved heart function in post myocardial infarction rats.Acta Biomater. 2025 Jan 15;192:235-247. doi: 10.1016/j.actbio.2024.12.009. Epub 2024 Dec 4. Acta Biomater. 2025. PMID: 39643223
-
Advancements in left ventricular assist devices to prevent pump thrombosis and blood coagulopathy.J Anat. 2023 Jan;242(1):29-49. doi: 10.1111/joa.13675. Epub 2022 Apr 20. J Anat. 2023. PMID: 35445389 Free PMC article. Review.
-
Soft Robotics.Biomimetics (Basel). 2019 Mar 12;4(1):22. doi: 10.3390/biomimetics4010022. Biomimetics (Basel). 2019. PMID: 31105207 Free PMC article.
-
Mechanical Characterization of 3D-Printed Patterned Membranes for Cardiac Tissue Engineering: An Experimental and Numerical Study.Biomedicines. 2023 Mar 21;11(3):963. doi: 10.3390/biomedicines11030963. Biomedicines. 2023. PMID: 36979942 Free PMC article.
References
-
- Benjamin E.J., Virani S.S., Callaway C.W., Chamberlain A.M., Chang A.R., Cheng S., Chiuve S.E., Cushman M., Delling F.N., Deo R., et al. Heart disease and stroke statistics—2018 Update: A report from the American Heart Association. Circulation. 2018;137:e67–e492. doi: 10.1161/CIR.0000000000000558. - DOI - PubMed
-
- Clarke S.A., Ghanta R.K., Ailawadi G., Holmes J.W. Stud Mechanobiol Tissue Eng Biomater. Springer-Verlag; Berlin/Heidelberg, Germany: Cardiac restraint and support following myocardial infarction; pp. 15 and 169–206. 2013/2014.
Publication types
LinkOut - more resources
Full Text Sources
