

Targeted Versus Continuous Delivery of Volatile Anesthetics During Cholinergic Bronchoconstriction
- PMID: 31106293
- PMCID: PMC6516463
- DOI: 10.1115/1.4040001
Targeted Versus Continuous Delivery of Volatile Anesthetics During Cholinergic Bronchoconstriction
Abstract
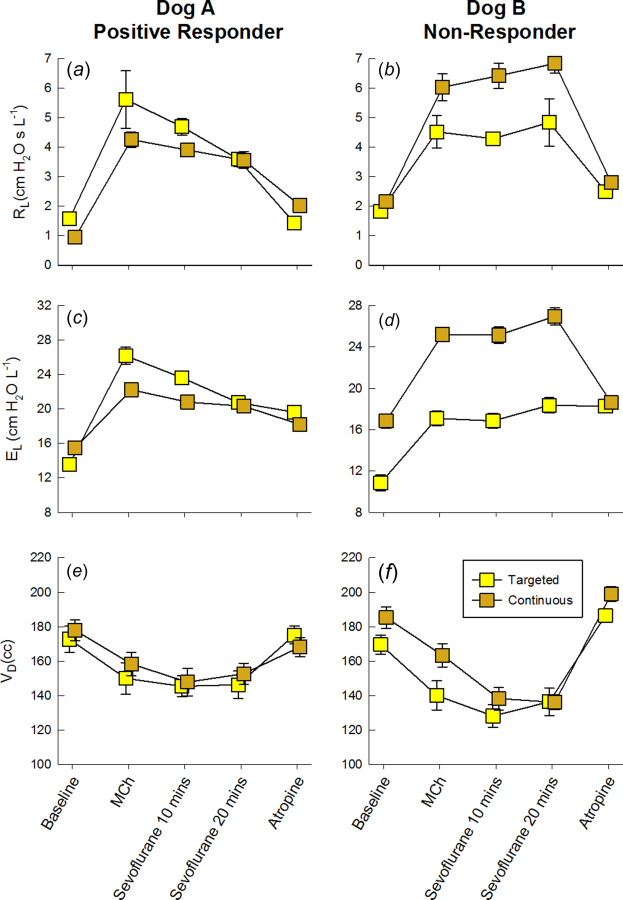
Volatile anesthetics have been shown to reduce lung resistance through dilation of constricted airways. In this study, we hypothesized that that diffusion of inhaled anesthetics from airway lumen to smooth muscle would yield significant bronchodilation in vivo, and systemic recirculation would not be necessary to reduce lung resistance (RL ) and elastance (EL ) during sustained bronchoconstriction. To test this hypothesis, we designed a delivery system for precise timing of inhaled volatile anesthetics during the course of a positive pressure breath. We compared changes in RL , EL , and anatomic dead space (VD ) in canines (N=5) during pharmacologically-induced bronchoconstriction with intravenous methacholine, and following treatments with: 1) targeted anesthetic delivery to VD ; and 2) continuous anesthetic delivery throughout inspiration. Both sevoflurane and isoflurane were used during each delivery regimen. Compared to continuous delivery, targeted delivery resulted in significantly lower doses of delivered anesthetic and decreased end-expiratory concentrations. However, we did not detect significant reductions in RL or EL for either anesthetic delivery regimen. This lack of response may have resulted from an insufficient dose of the anesthetic to cause bronchodilation, or from the preferential distribution of air flow with inhaled anesthetic delivery to less constricted, unobstructed regions of the lung, thereby enhancing airway heterogeneity and increasing apparent RL and EL .
Conflict of interest statement
CONFLICTS OF INTEREST Authors DWK, JRM, and BAS are listed as inventors on U.S. Patent Application Number US2015/0290418 A1
Figures







Similar articles
-
[Standard technical specifications for methacholine chloride (Methacholine) bronchial challenge test (2023)].Zhonghua Jie He He Hu Xi Za Zhi. 2024 Feb 12;47(2):101-119. doi: 10.3760/cma.j.cn112147-20231019-00247. Zhonghua Jie He He Hu Xi Za Zhi. 2024. PMID: 38309959 Chinese.
-
The protective effects of volatile anesthestics against the bronchoconstriction induced by an allergic reaction in sensitized rabbit pups.Anesth Analg. 2013 Jun;116(6):1257-64. doi: 10.1213/ANE.0b013e31828e5ccf. Epub 2013 Apr 16. Anesth Analg. 2013. PMID: 23592610
-
Temporal dynamics of acute isovolume bronchoconstriction in the rat.J Appl Physiol (1985). 1997 Jan;82(1):55-62. doi: 10.1152/jappl.1997.82.1.55. J Appl Physiol (1985). 1997. PMID: 9029198
-
Protective effects of volatile agents against methacholine-induced bronchoconstriction in rats.Anesthesiology. 2001 Feb;94(2):348-53. doi: 10.1097/00000542-200102000-00026. Anesthesiology. 2001. PMID: 11176101
-
Advanced technologies and devices for inhalational anesthetic drug dosing.Handb Exp Pharmacol. 2008;(182):451-70. doi: 10.1007/978-3-540-74806-9_21. Handb Exp Pharmacol. 2008. PMID: 18175104 Review.
Cited by
-
Positron Emission Tomography-Computed Tomography Imaging of Selective Lobar Delivery of Stem Cells in Ex Vivo Lung Model of Mechanical Ventilation.J Aerosol Med Pulm Drug Deliv. 2023 Feb;36(1):20-26. doi: 10.1089/jamp.2022.0013. Epub 2022 Dec 30. J Aerosol Med Pulm Drug Deliv. 2023. PMID: 36594924 Free PMC article.
-
Changes in lung mechanics and ventilation-perfusion match: comparison of pulmonary air- and thromboembolism in rats.BMC Pulm Med. 2024 Jan 10;24(1):27. doi: 10.1186/s12890-024-02842-z. BMC Pulm Med. 2024. PMID: 38200483 Free PMC article.
-
Assessment of Heterogeneity in Lung Structure and Function During Mechanical Ventilation: A Review of Methodologies.J Eng Sci Med Diagn Ther. 2022 Nov 1;5(4):040801. doi: 10.1115/1.4054386. Epub 2022 May 11. J Eng Sci Med Diagn Ther. 2022. PMID: 35832339 Free PMC article. Review.
References
-
- Meyer, N. E. , and Schotz, S. , 1939, “Relief of Severe Intractable Bronchial Asthma With Cyclopropane Anesthesia: Report of a Case,” J. Allergy, 10(3), pp. 239–240.10.1016/S0021-8707(39)90472-7 - DOI
-
- Schultz, T. E. , 2005, “Sevoflurane Administration in Status Asthmaticus: A Case Report,” AANA J., 73(1), pp. 35–36.https://www.ncbi.nlm.nih.gov/pubmed/15727281 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources