

Does the heart transplant have a future?
- PMID: 31106338
- PMCID: PMC6537946
- DOI: 10.1093/ejcts/ezz107
Does the heart transplant have a future?
Abstract
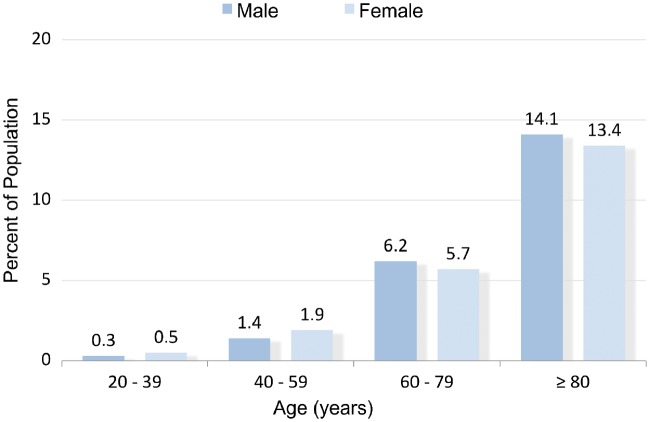
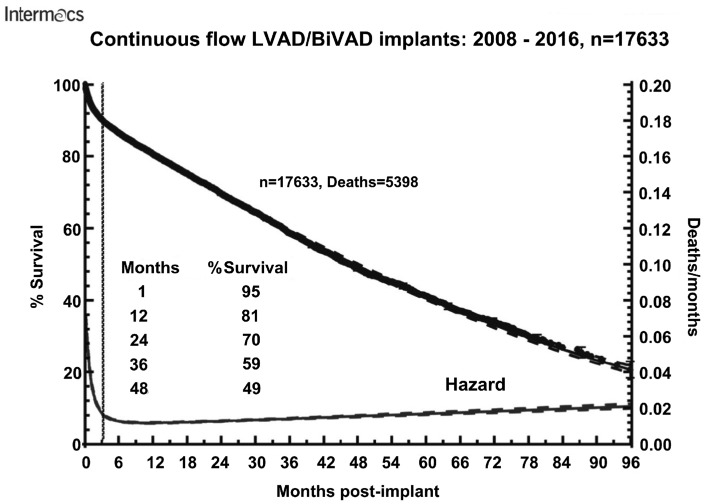
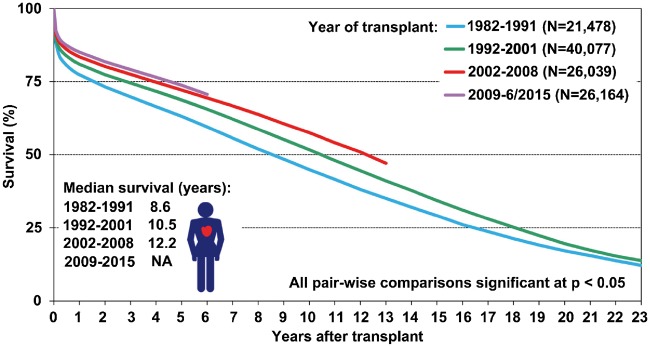
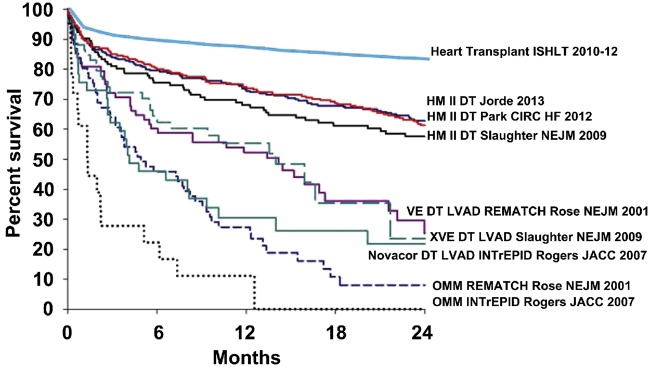
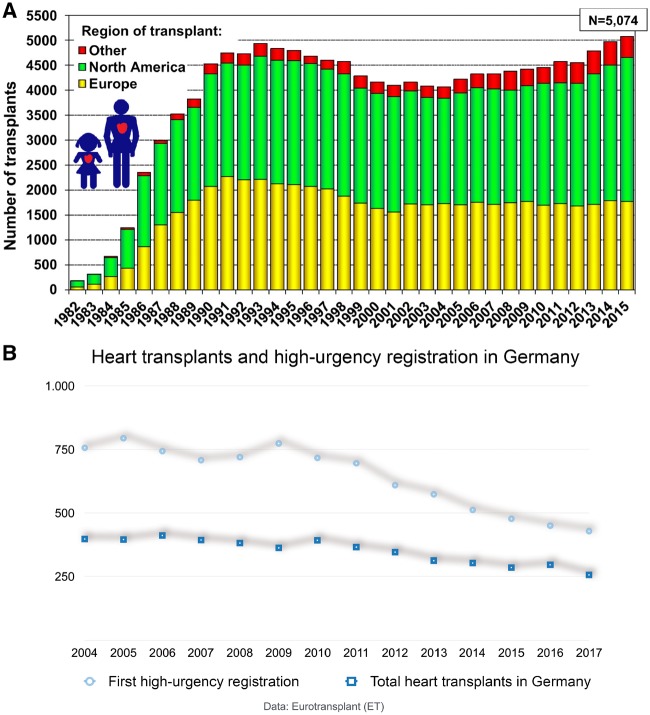
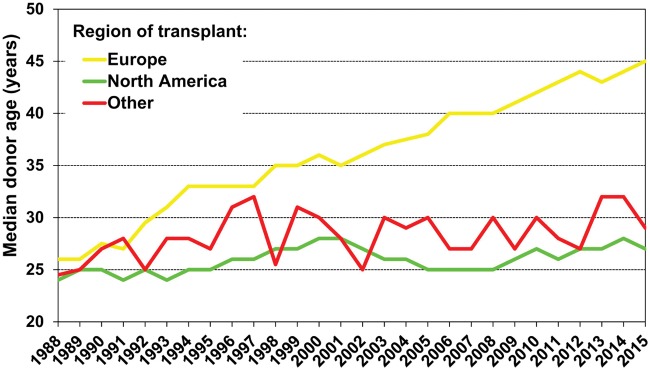
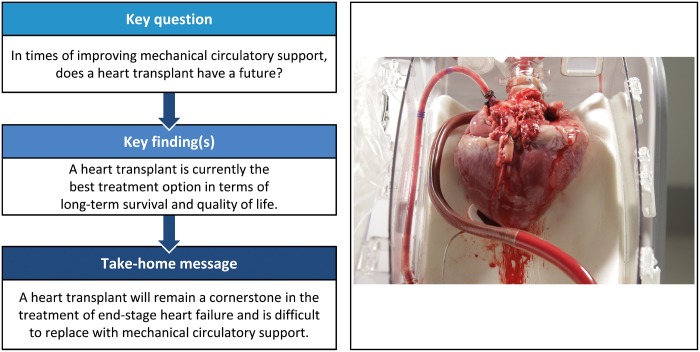
Heart failure has remained the leading cause of death globally for the last 15 years-and its prevalence will continue to rise. Fifty years ago, heart failure management was enriched by the possibility of a heart transplant. Despite impressive improvements in medical treatment for heart failure, a heart transplant remains the most effective long-lasting treatment for advanced heart failure in terms of mortality and quality of life. However, donor and recipient characteristics have changed dramatically in recent years, leading to more complex decision-making regarding organ acceptance and to more demanding operations and postoperative management. With improving pathophysiological understanding in the last decades, today's scientific interest still focuses on basic knowledge. How to retrieve and conserve organs to minimize ischaemic injury; how best to allocate them, considering the likelihood of success (developing a heart-allocation scoring system similar to that for lung allocation); how to match donor/recipient characteristics (ABO blood-group antigen compatibility versus incompatibility); and how to avoid graft failure, rejection and secondary morbidities such as malignomas and cardiac allograft vasculopathy after the heart transplant-all these factors remain fundamental challenges in today's transplant medicine. The use of ex vivo perfusion (e.g. via the Organ Care System®, TransMedics, Andover, MA, USA) may play an important role in this change. Remarkably, there are huge regional divergences in current transplant practices: Whereas the number of transplants continues to rise in most Eurotransplant countries and other major transplant networks, there are some countries in which transplant numbers are static or even dropping (as in Germany). This difference results in wide variations across different countries as to how advanced heart failure is treated using mechanical circulatory-assist devices.
Keywords: Heart failure; Heart transplant; Long-term survival; Mechanical circulatory support.
© The Author(s) 2019. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
References
-
- Ho KK, Pinsky JL, Kannel WB, Levy D.. The epidemiology of heart failure: the Framingham Study. J Am Coll Cardiol 1993;22:6A–13A. - PubMed
-
- Bleumink GS, Knetsch AM, Sturkenboom M, Straus S, Hofman A, Deckers JW. et al. Quantifying the heart failure epidemic: prevalence, incidence rate, lifetime risk and prognosis of heart failure: the Rotterdam Study. Eur Heart J 2004;25:1614–19. - PubMed
-
- Levy D, Larson MG, Vasan RS, Kannel WB, Ho KK.. The progression from hypertension to congestive heart failure. JAMA 1996;275:1557–62. - PubMed
-
- Fox KF, Cowie MR, Wood DA, Coats AJ, Gibbs JS, Underwood SR. et al. Coronary artery disease as the cause of incident heart failure in the population. Eur Heart J 2001;22:228–36. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
