

Clinical significance of BPI-ANCA detecting in COPD patients with Pseudomonas aeruginosa colonization
- PMID: 31106488
- PMCID: PMC6642326
- DOI: 10.1002/jcla.22908
Clinical significance of BPI-ANCA detecting in COPD patients with Pseudomonas aeruginosa colonization
Abstract
Background: Antineutrophil cytoplasmic autoantibodies against neutrophil granule bactericidal/permeability-increasing protein (BPI-ANCA) has been found in many inflammatory diseases, such as COPD, which can reduce the killing effect of BPI on Gram-negative bacteria. This study was aimed to assess the clinical significance of BPI-ANCA detecting in COPD patients with Pseudomonas aeruginosa (P aeruginosa) colonization.
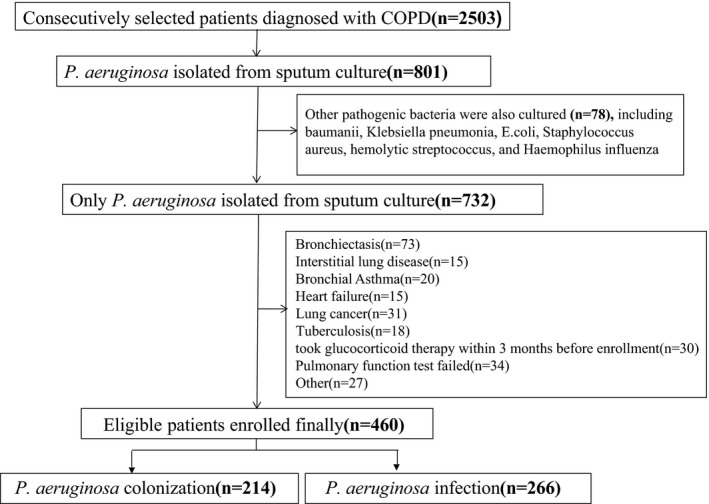
Methods: A total of 216 COPD patients with lung P aeruginosa colonization, 244 patients with P aeruginosa infection from June 2015 to June 2018, and 100 healthy individuals were included. Serum BPI-ANCA, tumor necrosis factor (TNF)-α, and interleukin (IL)-6 and IL-1β levels were detected by ELISA, and the lung function of the patients was measured at stable clinical stages. Patients with COPD were grouped according to BPI-ANCA detection and GOLD criteria, and serum TNF-α, IL-6, and IL-1β levels and indices reflecting lung function were compared and analyzed between groups.
Results: Positive rate of BPI-ANCA in COPD patients with P aeruginosa colonization was 48.15%; and compared with BPI-ANCA(-) group, FEV1 %pred and FEV1 /FVC(%) in BPI-ANCA(+) patients were significantly decreased, while TNF-α, IL-6, and IL-1β levels were elevated. There were 31.73% and 36.54% BPI-ANCA(+) patients with severe and very severe airflow limitation, respectively, which was significantly higher than that in the BPI-ANCA(-) group. FEV1 %pred and FEV1 /FVC(%) were negatively correlated with TNF-α, IL-6, IL-1β, and NEU%. C-reactive protein (CRP) was negatively correlated with FEV1 %pred, yet not significantly correlated with FEV1 /FVC(%).
Conclusion: BPI-ANCA positivity is associated with inflammatory status in COPD patients with pulmonary P aeruginosa colonization and can be used as a potential biomarker assessing disease severity.
Keywords: Pseudomonas aeruginosa; antineutrophil cytoplasm autoantibodies; bactericidal/permeability-increasing protein; chronic obstructive pulmonary disease; cytokines.
© 2019 The Authors. Journal of Clinical Laboratory Analysis Published by Wiley Periodicals, Inc.
Conflict of interest statement
All authors declared that they have no conflict of interests.
Figures
References
-
- Hassett DJ, Borchers MT, Panos RJ. Chronic obstructive pulmonary disease (COPD): evaluation from clinical, immunological and bacterial pathogenesis perspectives. J Microbiol. 2014;52:211‐226. - PubMed
-
- Vestbo J, Hurd SS, Agusti AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187:347‐365. - PubMed
-
- Canton R, Cobos N, de Gracia J, et al. Antimicrobial therapy for pulmonary pathogenic colonisation and infection by Pseudomonas aeruginosa in cystic fibrosis patients. Clin Microbiol Infect. 2005;11:690‐703. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
