

What Range of Motion and Functional Results Can Be Expected After Open Arthrolysis with Hinged External Fixation For Severe Posttraumatic Elbow Stiffness?
- PMID: 31107330
- PMCID: PMC6999955
- DOI: 10.1097/CORR.0000000000000726
What Range of Motion and Functional Results Can Be Expected After Open Arthrolysis with Hinged External Fixation For Severe Posttraumatic Elbow Stiffness?
Abstract
Background: The elbow is more susceptible to loss of motion after trauma than any other joint. Open arthrolysis often is performed for posttraumatic elbow stiffness if the stiffness does not improve with nonsurgical treatment, but the midterm results of this procedure and factors that may limit recovery have not been widely studied.
Questions/purposes: We reviewed patients who had undergone open arthrolysis with hinged external fixator for severe posttraumatic elbow stiffness (ROM ≤ 60°) with a minimum of 5 years followup to (1) analyze ROM gains; (2) assess functional improvement with the Mayo Elbow Performance Index (MEPI) and DASH, quality of life with the SF-36, pain with VAS, and ulnar nerve function with the Amadio rating scale and Dellon classification; and (3) identify complications and risk factors that might hinder mid-term elbow motion recovery after this procedure.
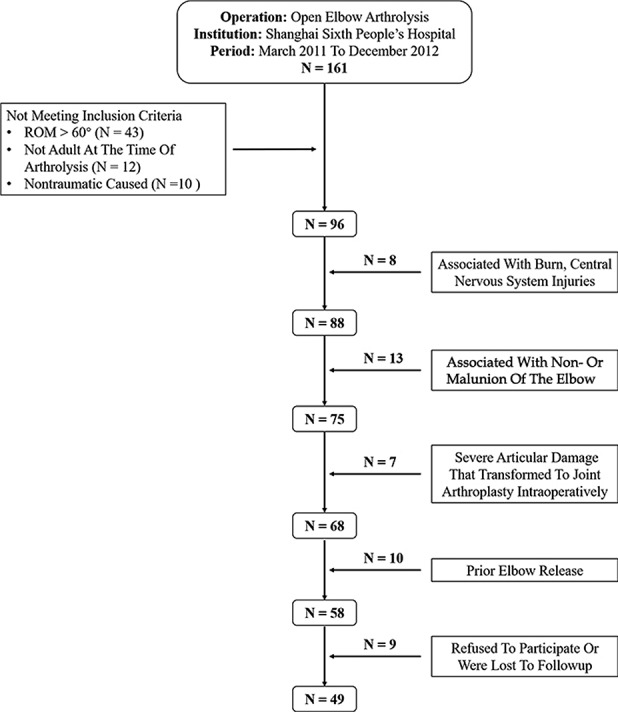
Methods: Between March 2011 and December 2012, we generally offered patients with elbow stiffness an open arthrolysis procedure when function did not improve with 6 months of nonoperative therapy, and no contraindications such as immature heterotopic ossification or complete destruction of articular cartilage were present. During that time, 161 patients underwent open arthrolysis for posttraumatic elbow stiffness at our institution; 49 of them satisfied the study inclusion criteria (adults with elbow ROM ≤ 60° as a result of trauma) and exclusion criteria (stiffness caused by burns or central nervous system injuries, causative trauma associated with nonunion or malunion of the elbow, severe articular damage that would have necessitated joint arthroplasty, or prior elbow release). In general, a combined medial-lateral approach to the elbow was performed to address the soft tissue tethers and any blocks to elbow motion, and a hinged external fixator was applied for 6 weeks to maintain elbow stability and improve the efficacy of postoperative rehabilitation. These patients were evaluated retrospectively at a mean followup period of 69 months (range, 62-83 months), and demographics, disease characteristics, arthrolysis details, pre- and postoutcome measures as noted, and complications were recorded via an electronic database. Multivariate regression analysis was performed to identify factors associated with ROM recovery.
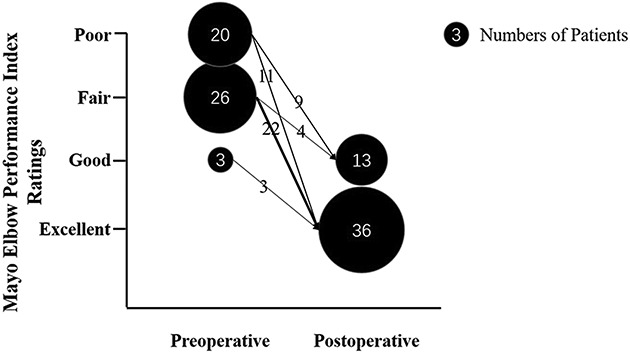
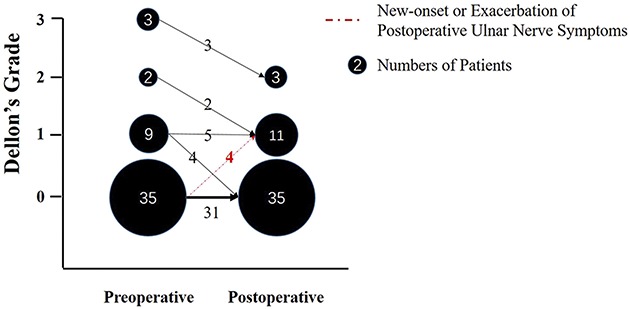
Results: At final followup, total ROM increased from a preoperative mean of 27 ± 20° to a postoperative mean of 131 ± 11° (mean difference, 104°; 95% CI, 98°-111°; p < 0.001), and 98% (48 of 49) of patients achieved a functional ROM of 30° to 130°. Improvements were also found in functional scores (MEPI: 54 ± 12 to 95 ± 7, mean difference, 41 points; DASH: 48 ± 17 to 8 ± 8, mean difference, 40 points; both p < 0.001), life quality (physical SF-36: 46 ± 11 to 81 ± 12, mean difference, 35 points; mental SF-36: 43 ± 14 to 80 ± 9, mean difference, 37 points; both p < .001), pain (VAS: 2.5 ± 2.4 to 0.4 ± 0.8; mean difference, 2.0 points; p < 0.001), and ulnar nerve function (Amadio score: 7.8 ± 1.9 to 8.4 ± 0.8; mean difference, 0.6 points; p = 0.004). A total of 18% (nine of 49 patients) developed complications, including new-onset or exacerbated nerve symptoms (four patients), recurrent heterotopic ossification (two patients), and pin-related infections (three patients). No patients underwent subsequent surgery for any of the above complications. Lastly, the medium-term ROM was divided into ROM ≤ 120° (n = 9) and ROM > 120° (n = 40). After controlling for potential confounding variables such as duration of stiffness and tobacco use, we found that tobacco use was the only independent risk factor examined (odds ratio, 9; 95% CI, 2-47; p = 0.009) associated with recovery of ROM.
Conclusions: Satisfactory medium-term results were found for open arthrolysis with hinged external fixation with our protocol in patients who had severe posttraumatic elbow stiffness. Appropriate and sufficient releases of tethered soft tissues and correction of any blocks that affect elbow motion intraoperatively, a dedicated team approach, and an aggressive and systematic postoperative rehabilitation program are the core steps for this procedure. Additionally, the importance of preoperative discontinuation of tobacco use should be emphasized.
Level of evidence: Level IV, therapeutic study.
Conflict of interest statement
All ICMJE Conflict of Interest Forms for authors and
Figures
References
-
- Amadio PC. Anatomical basis for a technique of ulnar nerve transposition. Surg Radiol Anat . 1986;8:155-161. - PubMed
-
- Blonna D, Wolf JM, Fitzsimmons JS, O'Driscoll SW. Prevention of nerve injury during arthroscopic capsulectomy of the elbow utilizing a safety-driven strategy. J Bone Joint Surg Am . 2013;95:1373-1381. - PubMed
-
- Briani RV, Ferreira AS, Pazzinatto MF, Pappas E, De Oliveira Silva D, Azevedo FM. What interventions can improve quality of life or psychosocial factors of individuals with knee osteoarthritis? A systematic review with meta-analysis of primary outcomes from randomised controlled trials. Br J Sports Med . 2018;52:1031-1038. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
