

Use of Viscoelastography in Malignancy-Associated Coagulopathy and Thrombosis: A Review
- PMID: 31108555
- PMCID: PMC7707018
- DOI: 10.1055/s-0039-1688497
Use of Viscoelastography in Malignancy-Associated Coagulopathy and Thrombosis: A Review
Abstract
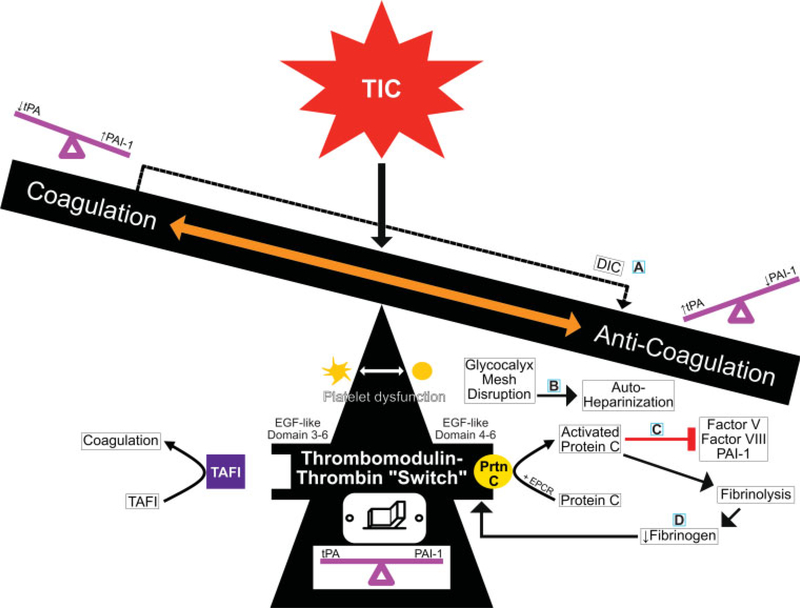
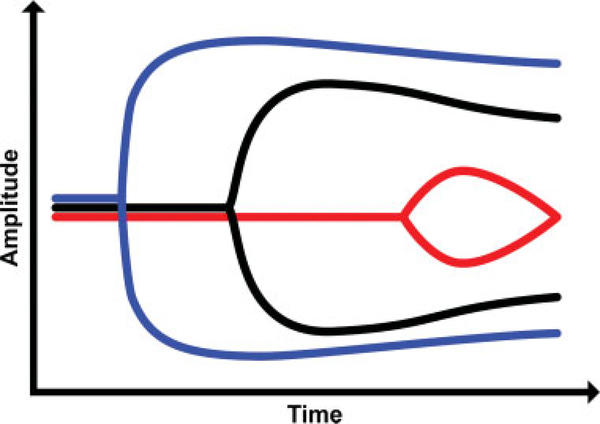
The relationship between malignancy and coagulopathy is one that is well documented yet incompletely understood. Clinicians have attempted to quantify the hypercoagulable state produced in various malignancies using common coagulation tests such as prothrombin time, activated partial thromboplastin time, and platelet count; however, due to these tests' focus on individual aspects of coagulation during one specific time point, they have failed to provide clinicians the complete picture of malignancy-associated coagulopathy (MAC). Viscoelastic tests (VETs), such as thromboelastography (TEG) and rotational thromboelastometry (ROTEM), are whole blood analyses that have the advantage of providing information related to the cumulative effects of plasma clotting factors, platelets, leukocytes, and red cells during all stages of the coagulation and fibrinolytic processes. VETs have gained popularity in the care of trauma patients to objectively measure trauma-induced coagulopathy (TIC), but the utility of VETs remains yet unrealized in many other medical specialties. The authors discuss the similarities and differences between TIC and MAC, and propose a mechanism for the hypercoagulable state of MAC that revolves around the thrombomodulin-thrombin complex as it switches between activating the protein C anticoagulation pathway or the thrombin activatable fibrinolysis inhibitor coagulation pathway. Additionally, they review the current literature on the use of TEG and ROTEM in patients with various malignancies. Although limited research is currently available, early results demonstrate the utility of both TEG and ROTEM in the prediction of hypercoagulable states and thromboembolic complications in oncologic patients.
Thieme Medical Publishers 333 Seventh Avenue, New York, NY 10001, USA.
Conflict of interest statement
Dr. Walsh reports grants from Haemonetics, outside the submitted work. Dr. H. Moore received research support from Instrument Laboratories and Haemonetics. He also shares intellectual property with Haemonetics and Thrombo Therapeutics Incorporated. He is also on the board of Thrombo Therapeutics Incorporated. Dr. E. Moore reports research grant from Haemonetics, outside the submitted work. In addition, he has a patent tPA TEG issued. Dr. Achneck reports having served as an employee of Haemonetics in the position of Director of Medical Affairs and Clinical Development during writing of the manuscript. The other authors have no conflict of interest to disclose.
Figures




Similar articles
-
Viscoelastic testing in oncology patients (including for the diagnosis of fibrinolysis): Review of existing evidence, technology comparison, and clinical utility.Transfusion. 2020 Oct;60 Suppl 6:S86-S100. doi: 10.1111/trf.16102. Transfusion. 2020. PMID: 33089937 Review.
-
A comparative study of tissue factor and kaolin on blood coagulation assays using rotational thromboelastometry and thromboelastography.Blood Coagul Fibrinolysis. 2016 Jan;27(1):31-41. doi: 10.1097/MBC.0000000000000381. Blood Coagul Fibrinolysis. 2016. PMID: 26340454
-
Targeted Thromboelastographic (TEG) Blood Component and Pharmacologic Hemostatic Therapy in Traumatic and Acquired Coagulopathy.Curr Drug Targets. 2016;17(8):954-70. doi: 10.2174/1389450117666160310153211. Curr Drug Targets. 2016. PMID: 26960340 Free PMC article. Review.
-
Thromboelastography.2023 Apr 10. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2023 Apr 10. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30725746 Free Books & Documents.
-
Thromboelastography and rotational thromboelastometry for the surgical intensivist: A narrative review.J Trauma Acute Care Surg. 2019 Apr;86(4):710-721. doi: 10.1097/TA.0000000000002206. J Trauma Acute Care Surg. 2019. PMID: 30633093 Free PMC article. Review.
Cited by
-
Analyzing venous thromboembolism risk in malignant tumors: thromboelastogram and coagulation factors study.Biomark Med. 2024;18(8):373-383. doi: 10.1080/17520363.2024.2342239. Epub 2024 Jun 4. Biomark Med. 2024. PMID: 39041842 Free PMC article.
-
Features of thromboelastogram in populations exposed to or transferring from high altitude.Heliyon. 2024 Jan 28;10(3):e25223. doi: 10.1016/j.heliyon.2024.e25223. eCollection 2024 Feb 15. Heliyon. 2024. PMID: 38322976 Free PMC article.
-
Evaluation of Haemostasis in Dogs Affected by Resectable Malignancy.Animals (Basel). 2022 Dec 31;13(1):164. doi: 10.3390/ani13010164. Animals (Basel). 2022. PMID: 36611772 Free PMC article.
-
Prediction model of gastrointestinal tumor malignancy based on coagulation indicators such as TEG and neural networks.Front Immunol. 2025 Mar 25;16:1507773. doi: 10.3389/fimmu.2025.1507773. eCollection 2025. Front Immunol. 2025. PMID: 40201179 Free PMC article.
-
"TEG" talks: technology worth spreading?Res Pract Thromb Haemost. 2023 Feb 28;7(1):100022. doi: 10.1016/j.rpth.2022.100022. eCollection 2023 Jan. Res Pract Thromb Haemost. 2023. PMID: 36970744 Free PMC article. No abstract available.
References
-
- Virchow RLK. Cellular Pathology: As Based upon Physiological and Pathological Histology. Twenty Lectures Delivered in the Pathological Institute of Berlin during the Months of February, March and April, 1858. New York, NY: RM De Witt; 1860 - PubMed
-
- Bagot CN, Arya R. Virchow and his triad: a question of attribution. Br J Haematol 2008;143(02):180–190 - PubMed
-
- Kashuk JL, Moore EE, Sabel A, et al. Rapid thrombelastography (r-TEG) identifies hypercoagulability and predicts thromboembolic events in surgical patients. Surgery 2009;146(04):764–772, discussion 772–774 - PubMed
-
- Trousseau A Clinique médicale de l’Hôtel-Dieu de Paris. Vol 2 Paris: Baillière; 1861
-
- Sørensen HT, Mellemkjaer L, Olsen JH, Baron JA. Prognosis of cancers associated with venous thromboembolism. N Engl J Med 2000;343(25):1846–1850 - PubMed
