

The effect of providing prescribing recommendations on appropriate prescribing: A cluster-randomized controlled trial in older adults in a preoperative setting
- PMID: 31108564
- PMCID: PMC6710520
- DOI: 10.1111/bcp.13987
The effect of providing prescribing recommendations on appropriate prescribing: A cluster-randomized controlled trial in older adults in a preoperative setting
Abstract
Aims: The Systematic Tool to Reduce Inappropriate Prescribing is a method to assess patient's medication and has been incorporated into a clinical decision support system: STRIP Assistant. Our aim was to evaluate the effect of recommendations generated using STRIP Assistant on appropriate prescribing and mortality in a preoperative setting.
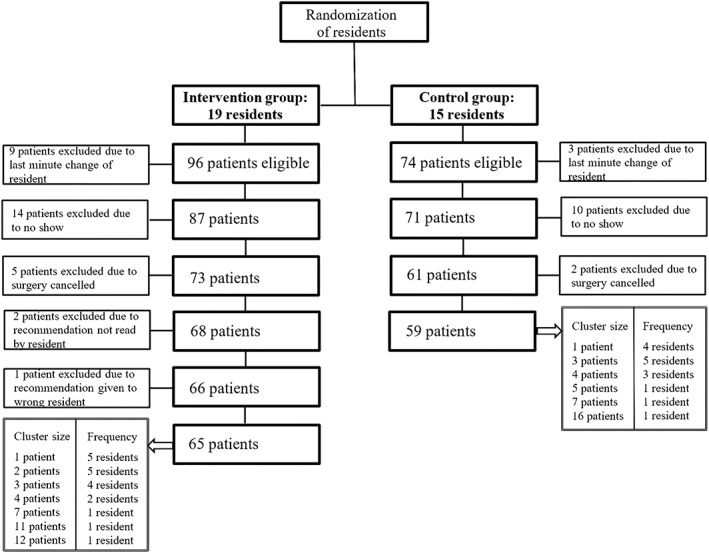
Methods: This cluster-randomized controlled trial was carried out at the preoperative geriatric outpatient clinic. Residents who performed a comprehensive geriatric assessment were randomized to the control group and intervention group in a 1:1 ratio. Visiting patients aged 70 years or older on 5 or more medications were included.
Intervention: prescribing recommendations were generated by a physician using STRIP Assistant and given to the resident. Control group residents performed a medication review according to usual care.
Primary outcome: number of medication changes made because of potential prescribing omissions (PPOs), potentially inappropriate medications (PIMs), and suboptimal dosages according to the prescribing recommendations. Secondary outcome: 3-month postoperative mortality.
Results: 65 intervention and 59 control patients were included, attended by 34 residents. Significantly more medication changes because of PPOs and PIMs were made in the intervention group than in the control group (PPOs 26.2% vs 3.4%, odds ratio 0.04 [95% confidence interval 0.003-0.46] P < .05; PIMS 46.2% vs 15.3% odds ratio 0.14 [95% confidence interval 0.07-0.57] P < .005). There were no differences in dose adjustments or in postoperative mortality.
Conclusion: Prescribing recommendations generated with the help of STRIP Assistant improved appropriate prescribing in a preoperative geriatric outpatient clinic but did not affect postoperative mortality.
Keywords: clinical pharmacology; clinical pharmacology, clinical trials; elderly; geriatrics, drug safety; geriatrics, geriatric medicine; prescribing.
© 2019 The Authors. British Journal of Clinical Pharmacology published by John Wiley & Sons Ltd on behalf of British Pharmacological Society.
Conflict of interest statement
There are no competing interests to declare.
Figures

References
-
- Leendertse AJ, Egberts ACG, Stoker LJ, van den Bemt P, HARM Study Group . Frequency of and risk factors for preventable medication‐related hospital admissions in the Netherlands. Arch Intern Med. 2008;168(17):1890–1896. - PubMed
-
- Hamilton H, Gallagher P, Ryan C, Byrne S, O'Mahony D. Potentially inappropriate medications defined by STOPP criteria and the risk of adverse drug events in older hospitalized patients. Arch Intern Med. 2011;171(11):1013–1019. - PubMed
-
- Padro Cabello AJ, Del Pozo Gavilán E, Gómez Jiménez FJ, et al. Drug‐related mortality among inpatients: a retrospective observational study. Eur J Clin Pharmacol. 2016;72(6):731–736. - PubMed
-
- Beijer HJ, de Blaey CJ. Hospitalisations caused by adverse drug reactions (ADR): a meta‐analysis of observational studies. Pharm World Sci. 2002;2:46–54. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
