

Left Ventricular Flow Analysis
- PMID: 31109184
- PMCID: PMC6544522
- DOI: 10.1161/CIRCIMAGING.118.008130
Left Ventricular Flow Analysis
Abstract
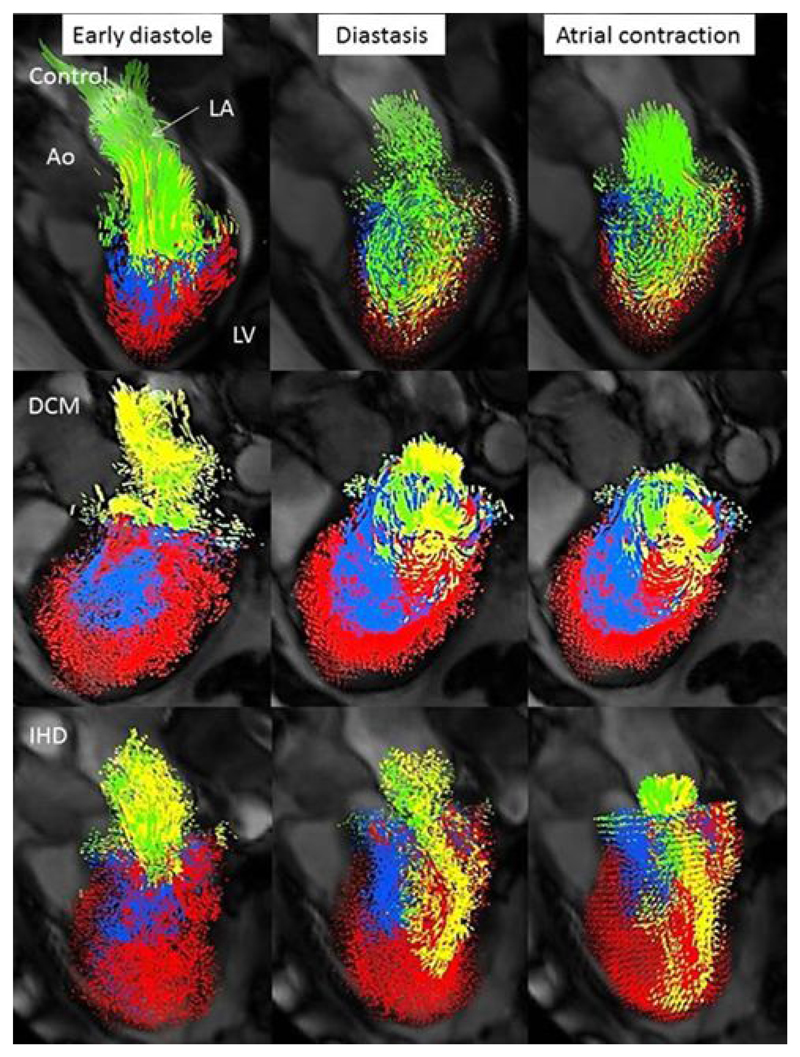
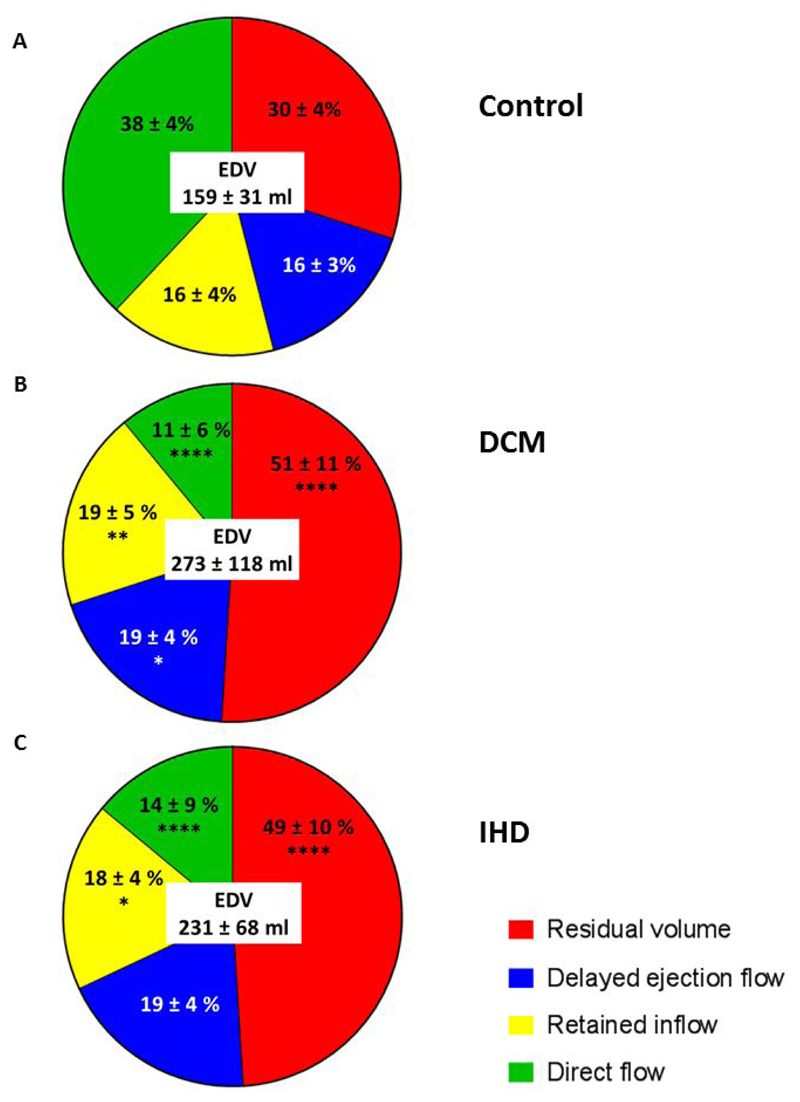
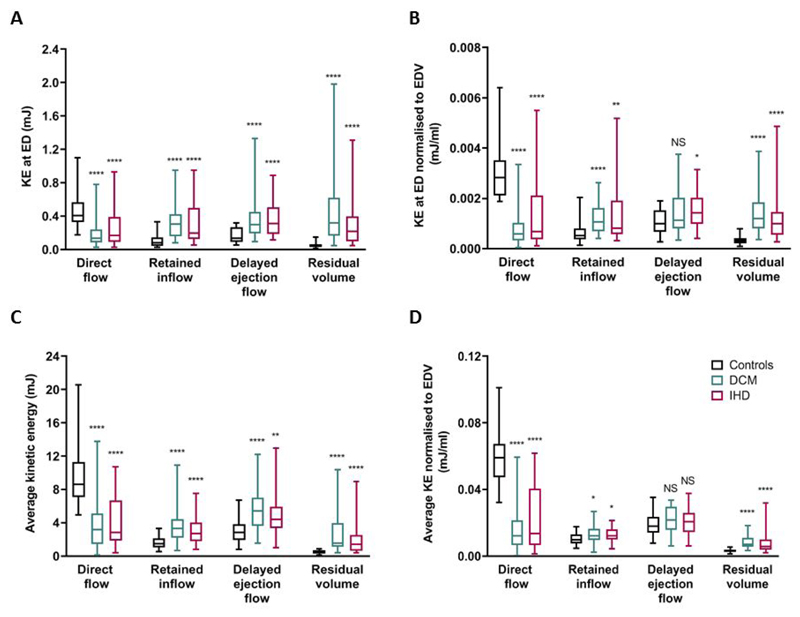
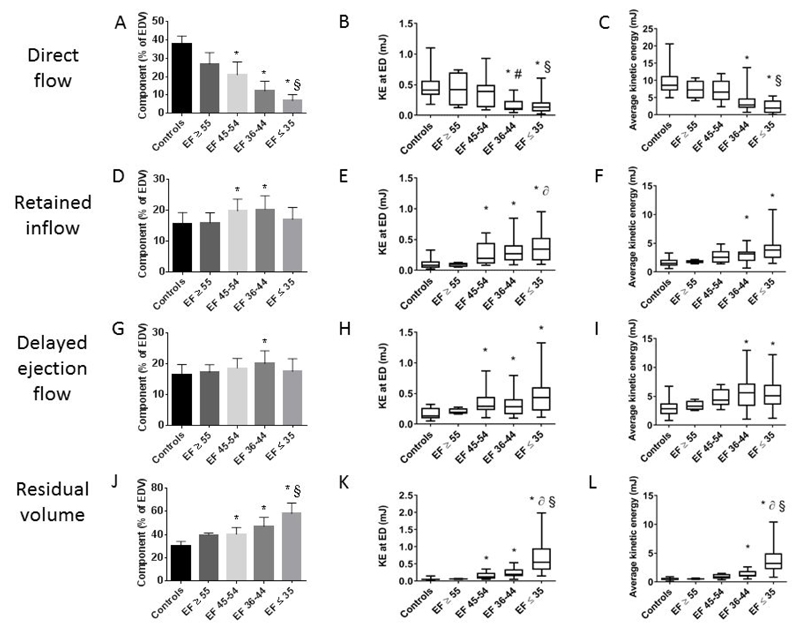
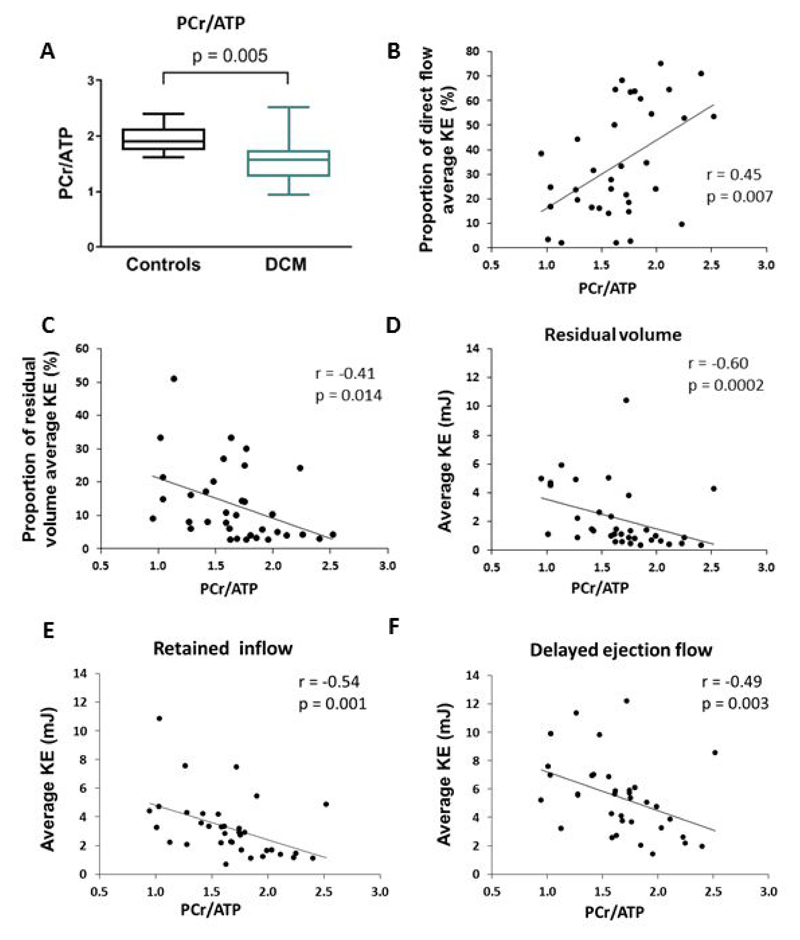
Background: Cardiac remodeling, after a myocardial insult, often causes progression to heart failure. The relationship between alterations in left ventricular blood flow, including kinetic energy (KE), and remodeling is uncertain. We hypothesized that increasing derangements in left ventricular blood flow would relate to (1) conventional cardiac remodeling markers, (2) increased levels of biochemical remodeling markers, (3) altered cardiac energetics, and (4) worsening patient symptoms and functional capacity. Methods Thirty-four dilated cardiomyopathy patients, 30 ischemic cardiomyopathy patients, and 36 controls underwent magnetic resonance including 4-dimensional flow, BNP (brain-type natriuretic peptide) measurement, functional capacity assessment (6-minute walk test), and symptom quantification. A subgroup of dilated cardiomyopathy and control subjects underwent cardiac energetic assessment. Left ventricular flow was separated into 4 components: direct flow, retained inflow, delayed ejection flow, and residual volume. Average KE throughout the cardiac cycle was calculated.
Results: Patients had reduced direct flow proportion and direct-flow average KE compared with controls ( P<0.0001). The residual volume proportion and residual volume average KE were increased in patients ( P<0.0001). Importantly, in a multiple linear regression model to predict the patient's 6-minute walk test, the independent predictors were age (β=-0.3015; P=0.019) and direct-flow average KE (β=0.280, P=0.035; R2 model, 0.466, P=0.002). In contrast, neither ejection fraction nor left ventricular volumes were independently predictive.
Conclusions: This study demonstrates an independent predictive relationship between the direct-flow average KE and a prognostic measure of functional capacity. Intracardiac 4-dimensional flow parameters are novel biomarkers in heart failure and may provide additive value in monitoring new therapies and predicting prognosis.
Keywords: biomarkers; heart failure; magnetic resonance imaging; prognosis; walk test.
Figures
Comment in
-
Unraveling the Complex Processes of Adverse Cardiac Remodeling.Circ Cardiovasc Imaging. 2019 May;12(5):e009086. doi: 10.1161/CIRCIMAGING.119.009086. Circ Cardiovasc Imaging. 2019. PMID: 31109183 No abstract available.
