

Acute kidney injury is associated with impaired cognition and chronic kidney disease in a prospective cohort of children with severe malaria
- PMID: 31109328
- PMCID: PMC6528242
- DOI: 10.1186/s12916-019-1332-7
Acute kidney injury is associated with impaired cognition and chronic kidney disease in a prospective cohort of children with severe malaria
Abstract
Background: Acute kidney injury (AKI) is a recognized complication of pediatric severe malaria, but its long-term consequences are unknown.
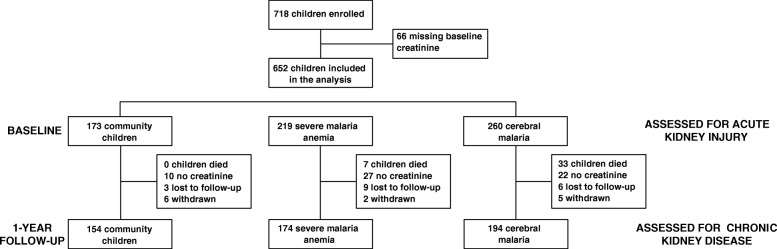
Methods: Ugandan children with cerebral malaria (CM, n = 260) and severe malaria anemia (SMA, n = 219) or community children (CC, n = 173) between 1.5 and 12 years of age were enrolled in a prospective cohort study. Kidney Disease: Improving Global Outcomes (KDIGO) criteria were used to retrospectively define AKI and chronic kidney disease (CKD). Cognitive testing was conducted using the Mullen Scales of Early Learning in children < 5 and Kaufman Assessment Battery for Children (K-ABC) second edition in children ≥ 5 years of age.
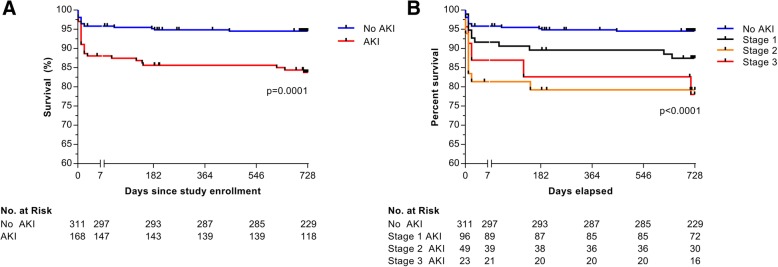
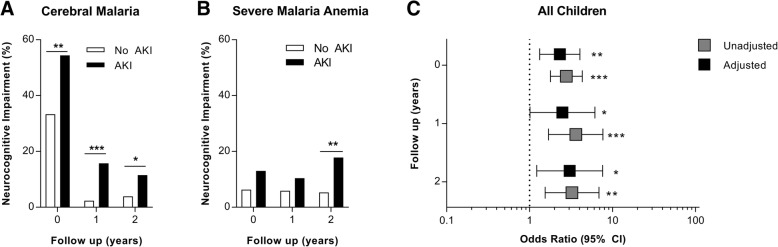
Results: The prevalence of AKI was 35.1%, ranging from 25.1% in SMA to 43.5% in CM. In-hospital mortality was 11.9% in AKI compared to 4.2% in children without AKI (p = 0.001), and post-discharge mortality was 4.7% in AKI compared to 1.3% in children without AKI (p = 0.030) corresponding to an all-cause adjusted hazard ratio of 2.30 (95% CI 1.21, 4.35). AKI was a risk factor for short- and long-term neurocognitive impairment. At 1 week post-discharge, the frequency of neurocognitive impairment was 37.3% in AKI compared to 13.5% in children without AKI (adjusted odds ratio (aOR) 2.31 [95% CI 1.32, 4.04]); at 1-year follow-up, it was 13.3% in AKI compared to 3.4% in children without AKI (aOR 2.48 [95% CI 1.01, 6.10]), and at 2-year follow-up, it was 13.0% in AKI compared to 3.4% in children without AKI (aOR 3.03 [95% CI 1.22, 7.58]). AKI was a risk factor for CKD at 1-year follow-up: 7.6% of children with severe malaria-associated AKI had CKD at follow-up compared to 2.8% of children without AKI (p = 0.038) corresponding to an OR of 2.81 (95% CI 1.02, 7.73). The presenting etiology of AKI was consistent with prerenal azotemia, and lactate dehydrogenase as a marker of intravascular hemolysis was an independent risk factor for AKI in CM and SMA (p < 0.0001). In CM, AKI was associated with the presence and severity of retinopathy (p < 0.05) and increased cerebrospinal fluid albumin suggestive of blood-brain barrier disruption.
Conclusions: AKI is a risk factor for long-term neurocognitive impairment and CKD in pediatric severe malaria.
Keywords: Acute kidney injury; Child; Chronic kidney disease; Cognition; Malaria; Mortality.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- WHO . World malaria report 2018. Geneva: World Health Organization; 2018.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
