

Tumor-to-tumor metastasis: a rare case of breast carcinoma metastasizing to a pheochromocytoma, and a literature review
- PMID: 31109373
- PMCID: PMC6528332
- DOI: 10.1186/s13000-019-0816-2
Tumor-to-tumor metastasis: a rare case of breast carcinoma metastasizing to a pheochromocytoma, and a literature review
Abstract
Background: Tumor-to-tumor metastasis is a well-recognized but uncommon entity. Breast carcinoma is one of the most common metastatic donors. Breast carcinoma metastasizes commonly to adrenal glands. However, the co-existence of a metastatic lesion with an existing adrenal tumor is a rare finding.
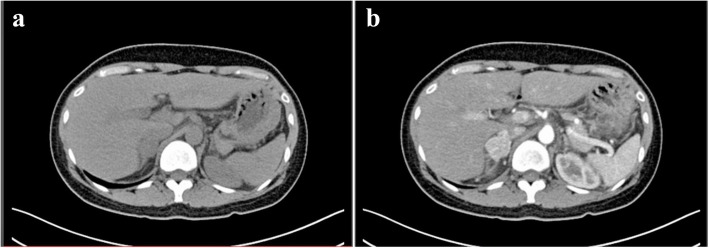
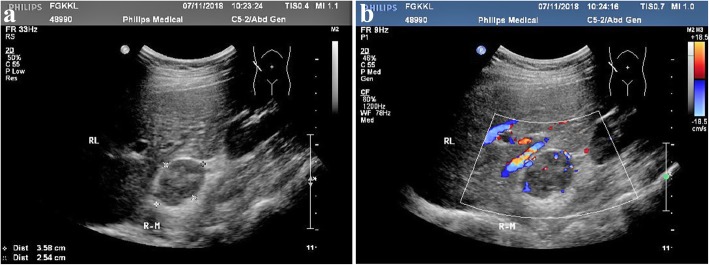
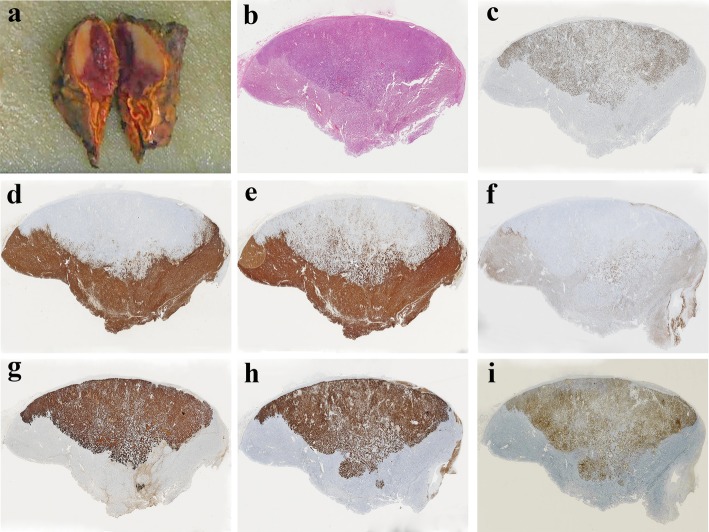
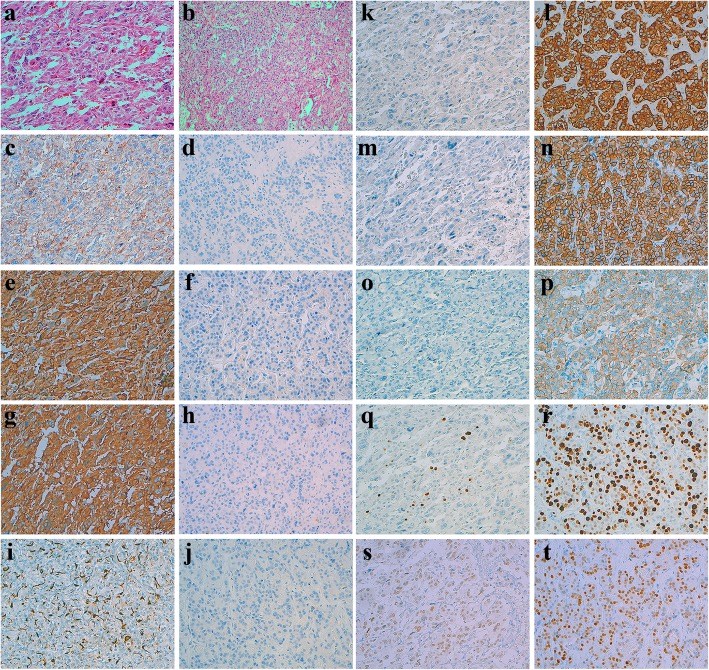
Case presentation: A 35-year-old woman was diagnosed with pheochromocytoma using computed tomography and ultrasound examinations. The tumor was surgically removed. Histological and immunohistochemical staining suggested that there were two components in the tumor: pheochromocytoma and metastatic cancer.
Conclusion: This is the second published case of pheochromocytoma with tumor-to-tumor metastasis from an invasive ductal carcinoma of the breast. Furthermore, we highlight the importance of awareness of tumor-to-tumor metastasis in pathological diagnosis.
Keywords: Breast carcinoma; Pheochromocytoma; Tumor-to-tumor metastasis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
