

Right ventricular-vascular coupling ratio in pediatric pulmonary arterial hypertension: A comparison between cardiac magnetic resonance and right heart catheterization measurements
- PMID: 31109778
- PMCID: PMC6710117
- DOI: 10.1016/j.ijcard.2019.05.021
Right ventricular-vascular coupling ratio in pediatric pulmonary arterial hypertension: A comparison between cardiac magnetic resonance and right heart catheterization measurements
Abstract
Background: In pulmonary arterial hypertension (PAH), right ventricular (RV) failure is the main cause of mortality. Non-invasive estimation of ventricular-vascular coupling ratio (VVCR), describing contractile response to afterload, could be a valuable tool for monitoring clinical course in children with PAH. This study aimed to test two hypotheses: VVCR by cardiac magnetic resonance (VVCRCMR) correlates with conventional VVCR by right heart catheterization (VVCRRHC) and both correlate with disease severity.
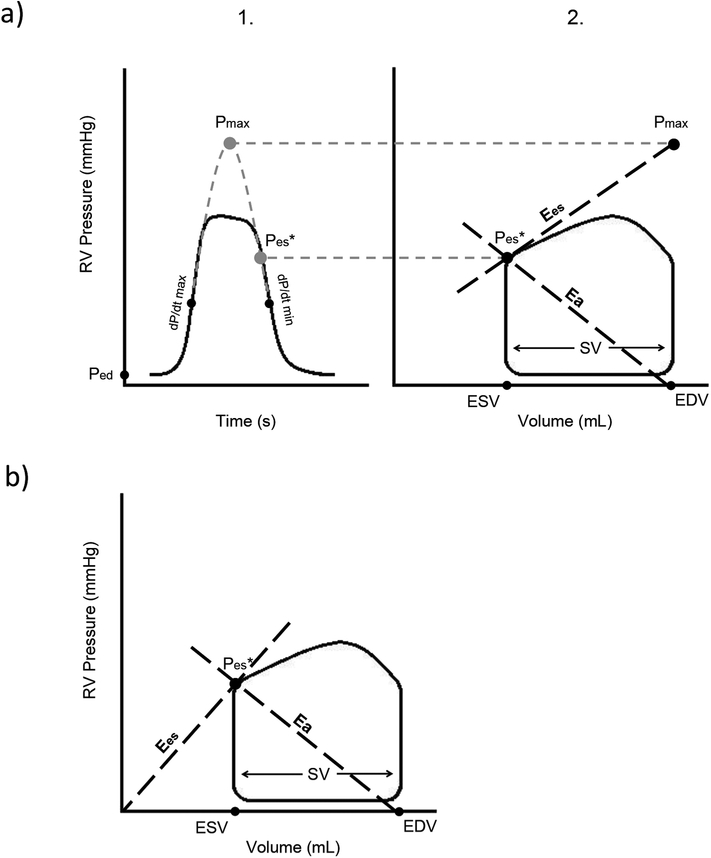
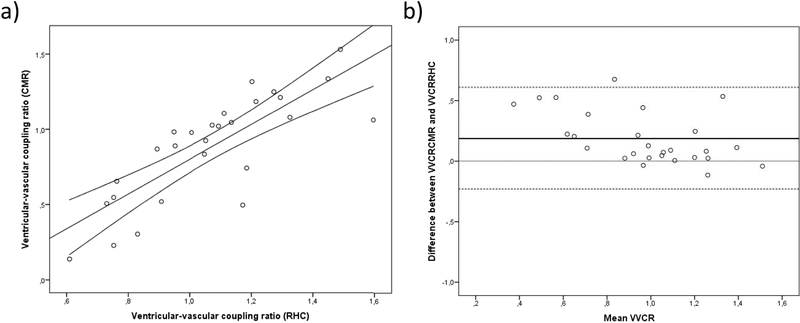
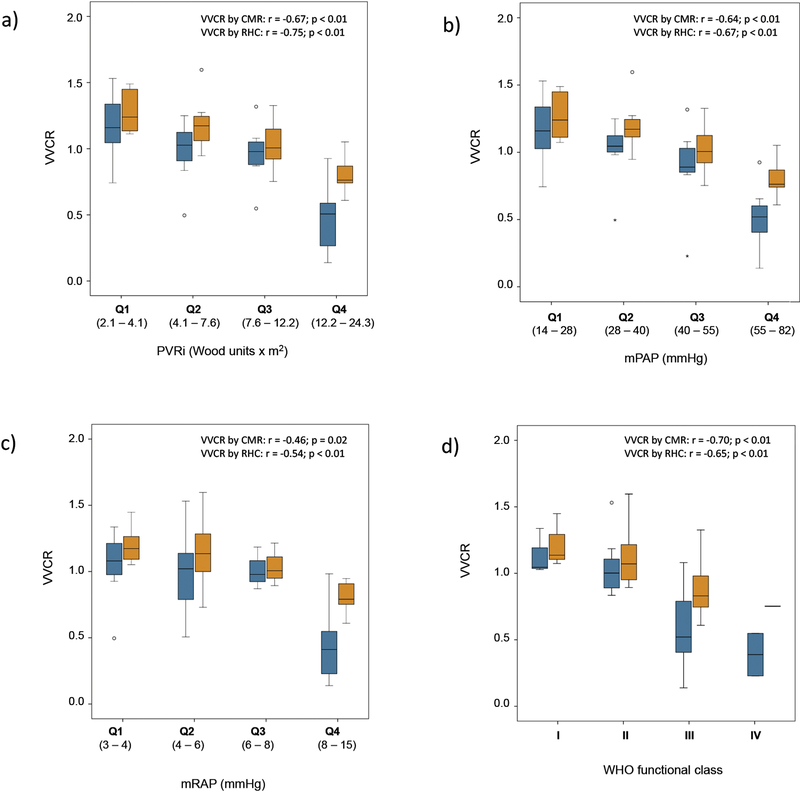
Methods and results: Twenty-seven patients diagnosed with idiopathic and associated PAH without post-tricuspid shunt, who underwent RHC and CMR within 17 days at two specialized centers for pediatric PAH were retrospectively studied. Clinical functional status and hemodynamic data were collected. Median age at time of MRI was 14.3 years (IQR: 11.1-16.8), median PVRi 7.6 WU × m2 (IQR: 4.1-12.2), median mPAP 40 mm Hg (IQR: 28-55) and median WHO-FC 2 (IQR: 2-3). VVCRCMR, defined as stroke volume/end-systolic volume ratio was compared to VVCRRHC by single-beat pressure method using correlation and Bland-Altman plots. VVCRCMR and VVCRRHC showed a strong correlation (r = 0.83, p < 0.001). VVCRCMR and VVCRRHC both correlated with clinical measures of disease severity (pulmonary vascular resistance index [PVRi], mean pulmonary artery pressure [mPAP], mean right atrial pressure [mRAP], and World Health Organization functional class [WHO-FC]; all p ≤ 0.02).
Conclusions: Non-invasively measured VVCRCMR is feasible in pediatric PAH and comparable to invasively assessed VVCRRHC. Both correlate with functional and hemodynamic measures of disease severity. The role of VVCR assessed by CMR and RHC in clinical decision-making and follow-up in pediatric PAH warrants further clinical investigation.
Keywords: Cardiac magnetic resonance; Pediatric pulmonary hypertension; Right heart catheterization; Right ventricular function; Ventricular-vascular coupling ratio.
Copyright © 2019 Elsevier B.V. All rights reserved.
Figures
Similar articles
-
Non-invasive determination by cardiovascular magnetic resonance of right ventricular-vascular coupling in children and adolescents with pulmonary hypertension.J Cardiovasc Magn Reson. 2015 Sep 16;17(1):81. doi: 10.1186/s12968-015-0186-1. J Cardiovasc Magn Reson. 2015. PMID: 26376972 Free PMC article.
-
Cardiovascular magnetic resonance-guided right heart catheterization in a conventional CMR environment - predictors of procedure success and duration in pulmonary artery hypertension.J Cardiovasc Magn Reson. 2019 Sep 9;21(1):57. doi: 10.1186/s12968-019-0569-9. J Cardiovasc Magn Reson. 2019. PMID: 31495338 Free PMC article.
-
Right ventricular stroke work index by echocardiography in adult patients with pulmonary arterial hypertension.BMC Cardiovasc Disord. 2021 Apr 30;21(1):219. doi: 10.1186/s12872-021-02037-y. BMC Cardiovasc Disord. 2021. PMID: 33931021 Free PMC article.
-
Cardiac Magnetic Resonance Imaging in Pulmonary Arterial Hypertension: Ready for Clinical Practice and Guidelines?Curr Heart Fail Rep. 2020 Oct;17(5):181-191. doi: 10.1007/s11897-020-00479-7. Curr Heart Fail Rep. 2020. PMID: 32870447 Free PMC article. Review.
-
Noninvasive Assessment of Right Ventricular Function in Patients with Pulmonary Arterial Hypertension and Left Ventricular Assist Device.Curr Cardiol Rep. 2019 Jul 5;21(8):82. doi: 10.1007/s11886-019-1156-2. Curr Cardiol Rep. 2019. PMID: 31278558 Review.
Cited by
-
Assessment and diagnosis of right ventricular failure-retrospection and future directions.Front Cardiovasc Med. 2023 May 30;10:1030864. doi: 10.3389/fcvm.2023.1030864. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37324632 Free PMC article. Review.
-
Role of cardiovascular magnetic resonance in pediatric pulmonary hypertension-novel concepts and imaging biomarkers.Cardiovasc Diagn Ther. 2021 Aug;11(4):1057-1069. doi: 10.21037/cdt-20-270. Cardiovasc Diagn Ther. 2021. PMID: 34527532 Free PMC article. Review.
-
A review on experimental surgical models and anesthetic protocols of heart failure in rats.Front Vet Sci. 2023 Mar 27;10:1103229. doi: 10.3389/fvets.2023.1103229. eCollection 2023. Front Vet Sci. 2023. PMID: 37051509 Free PMC article. Review.
-
Exercise right ventricular ejection fraction predicts right ventricular contractile reserve.J Heart Lung Transplant. 2021 Jun;40(6):504-512. doi: 10.1016/j.healun.2021.02.005. Epub 2021 Feb 17. J Heart Lung Transplant. 2021. PMID: 33752973 Free PMC article.
-
Mechanics of right ventricular dysfunction in pulmonary arterial hypertension and heart failure with preserved ejection fraction.Cardiovasc Diagn Ther. 2020 Oct;10(5):1580-1603. doi: 10.21037/cdt-20-479. Cardiovasc Diagn Ther. 2020. PMID: 33224775 Free PMC article. Review.
References
-
- D’Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med.1991;115(5):343–9. - PubMed
-
- Raymond RJ, Hinderliter AL, Iv PWW, Ralph D, Caldwell EJ, Williams W, et al. Echocardiographic predictors of adverse outcomes in primary pulmonary hypertension. J Am Coll Cardiol. 2002;39(7):1214–9. - PubMed
-
- Ploegstra MJ, Roofthooft MT, Douwes JM, Bartelds B, Elzenga NJ, van de Weerd D, et al. Echocardiography in pediatric pulmonary arterial hypertension: early study on assessing disease severity and predicting outcome. Circ Cardiovasc Imaging. 2015;8(1). pii: e000878. - PubMed
-
- Brierre G, Blot-Souletie N, Degano B, Tetu L, Bongard V, Carrie D. New echocardiographic prognostic factors for mortality in pulmonary arterial hypertension. Eur J Echocardiogr. 2010;11(6):516–22. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
