

Nonunions of the humerus - Treatment concepts and results of the last five years
- PMID: 31109830
- PMCID: PMC6667773
- DOI: 10.1016/j.cjtee.2019.04.002
Nonunions of the humerus - Treatment concepts and results of the last five years
Abstract
Purpose: Fractures of the humerus account for 5%-8% of all fractures. Nonunion is found with an incidence of up to 15%, depending on the location of the fracture. In case of a manifest nonunion the surgeon faces a challenging problem and has to conceive a therapy based on the underlying pathology. The aim of this study was to describe our treatment concepts for this entity and present our results of the last five years.
Methods: Twenty-six patients were treated for nonunion of the humerus between January 2013 and December 2017. Their charts were reviewed retrospectively and demographic data, pathology, surgical treatment and outcome were assessed.
Results: The most frequent location for a nonunion was the humeral shaft, with the most common trauma mechanism being multiple falls. Most often atrophic nonunion (n = 14), followed by hypertrophic and infection-caused nonunion (each n = 4), were found. Our treatment concept could be applied in 19 patients, of which in 90% of those who were available for follow-up consolidation could be achieved.
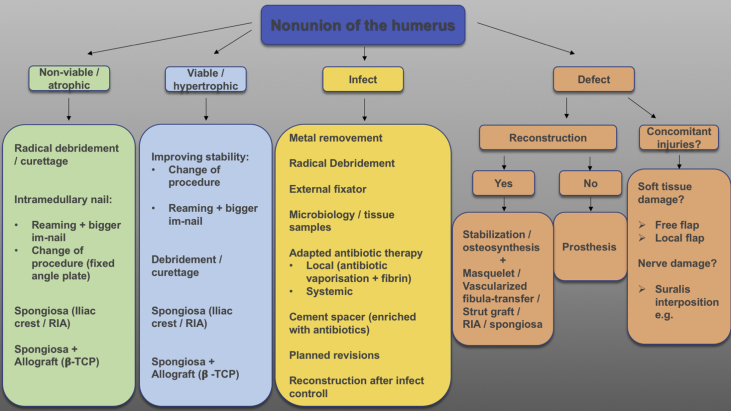
Conclusion: Humeral nonunion is a heterogeneous entity that has to be analyzed precisely and be treated correspondingly. We therefore present a treatment concept based on the underlying pathology.
Keywords: Delayed union; Humeral fractures; Humerus; Nonunion.
Copyright © 2019 Chinese Medical Association. Production and hosting by Elsevier B.V. All rights reserved.
Figures

References
-
- Volgas D.A., Stannard J.P., Alonso J.E. Nonunions of the humerus. Clin Orthop Relat Res. 2004;419:46–50. - PubMed
-
- Wenzl M.E., Porté Thomas, Fuchs Stefan. Verfahren zur rekonstruktion und osteosynthese von pseudarthrosen des humerus. Trauma Berufskrankh. 2003;5:s86–s91.
-
- Badman B.L., Mighell M., Kalandiak S.P. Proximal humeral nonunions treated with fixed-angle locked plating and an intramedullary strut allograft. J Orthop Trauma. 2009;23:173–179. - PubMed
-
- Weber B.G., Cech O. first ed. Hans Huber; Bern: 1973. Pseudarthrosen: Pathophysiologie, Biomechanik, Therapie, Ergebnisse; pp. 42–44.
-
- Rupp M., Biehl C., Budak M. Diaphyseal long bone nonunions - types, aetiology, economics, and treatment recommendations. Int Orthop. 2018;42:247–258. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical