

A Guide to Understanding Antimicrobial Drug Dosing in Critically Ill Patients on Renal Replacement Therapy
- PMID: 31109983
- PMCID: PMC6658763
- DOI: 10.1128/AAC.00583-19
A Guide to Understanding Antimicrobial Drug Dosing in Critically Ill Patients on Renal Replacement Therapy
Abstract
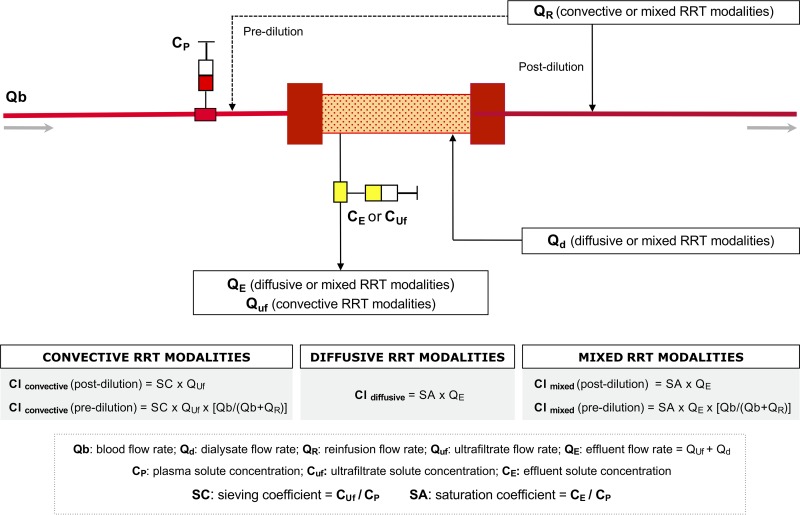
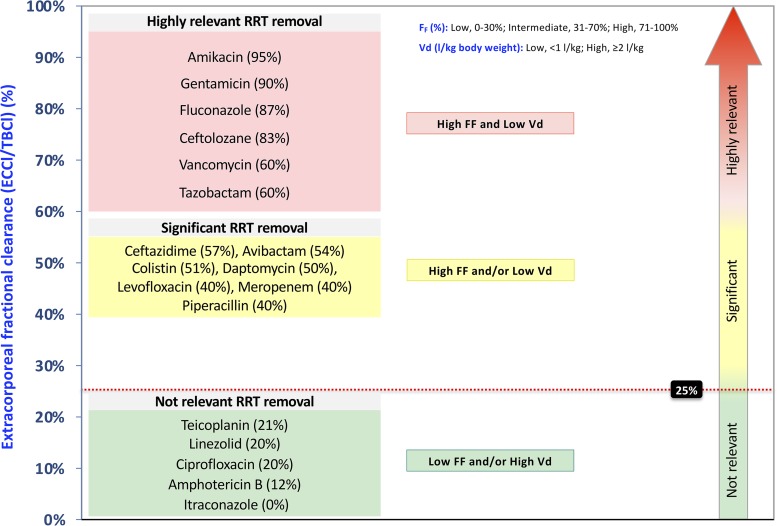
A careful management of antimicrobials is essential in the critically ill with acute kidney injury, especially if renal replacement therapy is required. Acute kidney injury may lead per se to clinically significant modifications of drugs' pharmacokinetic parameters, and the need for renal replacement therapy represents a further variable that should be considered to avoid inappropriate antimicrobial therapy. The most important pharmacokinetic parameters, useful to determine the significance of extracorporeal removal of a given drug, are molecular weight, protein binding, and distribution volume. In many cases, the extracorporeal removal of antimicrobials can be relevant, with a consistent risk of underdosing-related treatment failure and/or potential onset of bacterial resistance. It should also be taken into account that renal replacement therapies are often not standardized in critically ill patients, and their impact on plasma drug concentrations may substantially vary in relation to membrane characteristics, treatment modality, and delivered dialysis dose. Thus, in this clinical scenario, the knowledge of the pharmacokinetic and pharmacodynamic properties of different antimicrobial classes is crucial to tailor maintenance dose and/or time interval according to clinical needs. Finally, especially for antimicrobials known for a tight therapeutic range, therapeutic drug monitoring is strongly suggested to guide dosing adjustment in complex clinical settings, such as septic patients with acute kidney injury undergoing renal replacement therapy.
Keywords: CRRT; acute kidney injury; antimicrobials; continuous renal replacement therapy; convection; diffusion; extracorporeal clearance; pharmacodynamics; pharmacokinetics; renal replacement therapy.
Copyright © 2019 American Society for Microbiology.
Figures
References
-
- Mehta RL, Bouchard J, Soroko SB, Ikizler TA, Paganini EP, Chertow GM, Himmelfarb J, Program to Improve Care in Acute Renal Disease (PICARD) Study Group. 2011. Sepsis as a cause and consequence of acute kidney injury: Program to Improve Care in Acute Renal Disease. Intensive Care Med 37:241–248. doi: 10.1007/s00134-010-2089-9. - DOI - PMC - PubMed
-
- Kidney Disease Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. 2012. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int S2:1–138.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
