

A Phase I Dose-Escalation Trial of BN-CV301, a Recombinant Poxviral Vaccine Targeting MUC1 and CEA with Costimulatory Molecules
- PMID: 31110074
- PMCID: PMC6697621
- DOI: 10.1158/1078-0432.CCR-19-0183
A Phase I Dose-Escalation Trial of BN-CV301, a Recombinant Poxviral Vaccine Targeting MUC1 and CEA with Costimulatory Molecules
Abstract
Purpose: BN-CV301 is a poxviral-based vaccine comprised of recombinant (rec.) modified vaccinia Ankara (MVA-BN-CV301; prime) and rec. fowlpox (FPV-CV301; boost). Like its predecessor PANVAC, BN-CV301 contains transgenes encoding tumor-associated antigens MUC1 and CEA as well as costimulatory molecules (B7.1, ICAM-1, and LFA-3). PANVAC was reengineered to make it safer and more antigenic.
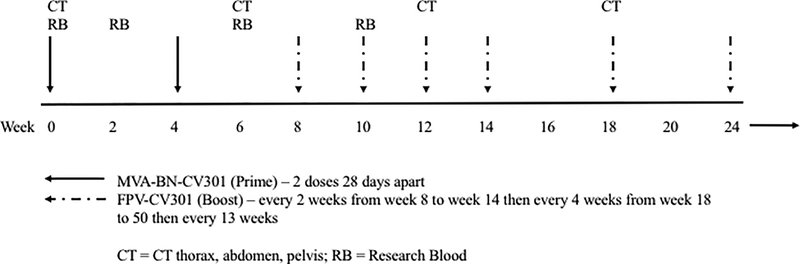
Patients and methods: This open-label, 3+3 design, dose-escalation trial evaluated three dose levels (DL) of MVA-BN-CV301: one, two, or four subcutaneous injections of 4 × 108 infectious units (Inf.U)/0.5 mL on weeks 0 and 4. All patients received FPV-CV301 subcutaneously at 1 × 109 Inf.U/0.5 mL every 2 weeks for 4 doses, then every 4 weeks. Clinical and immune responses were evaluated.
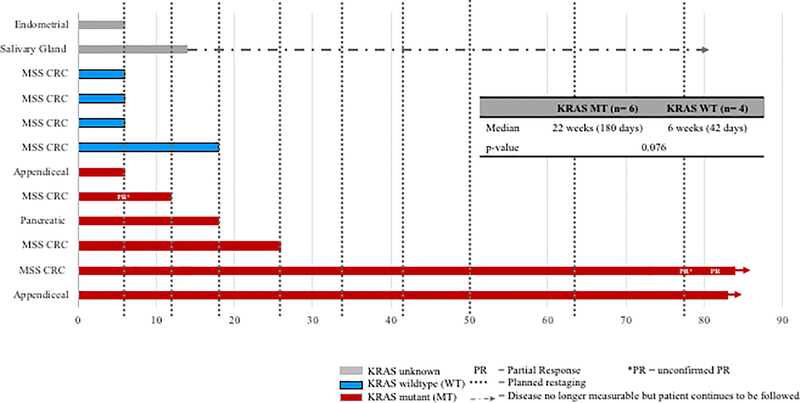
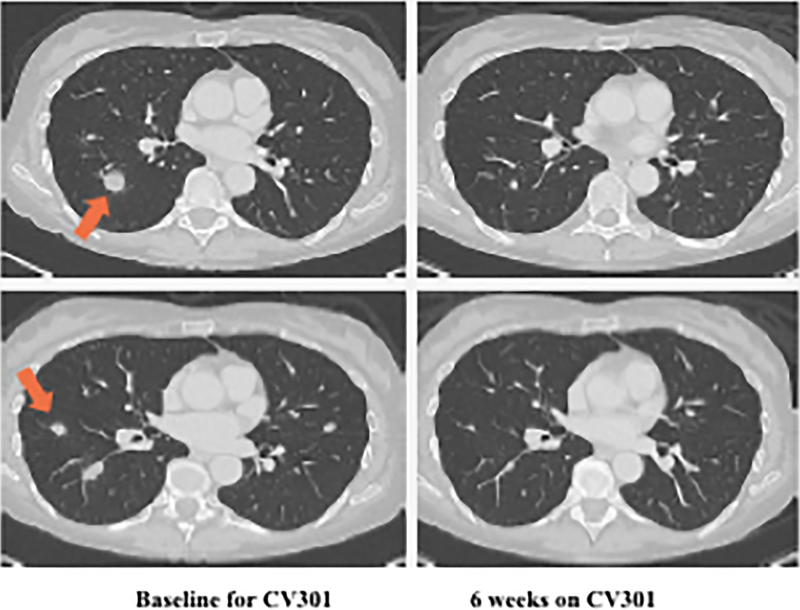
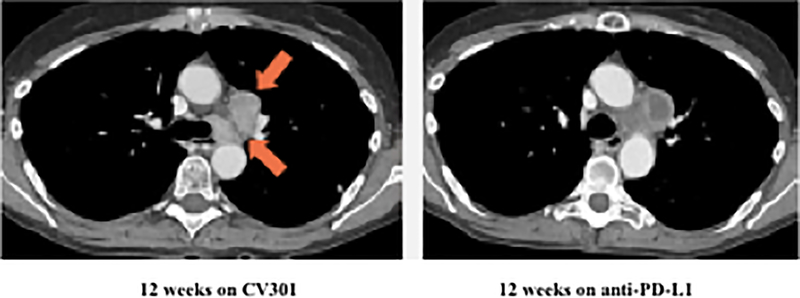
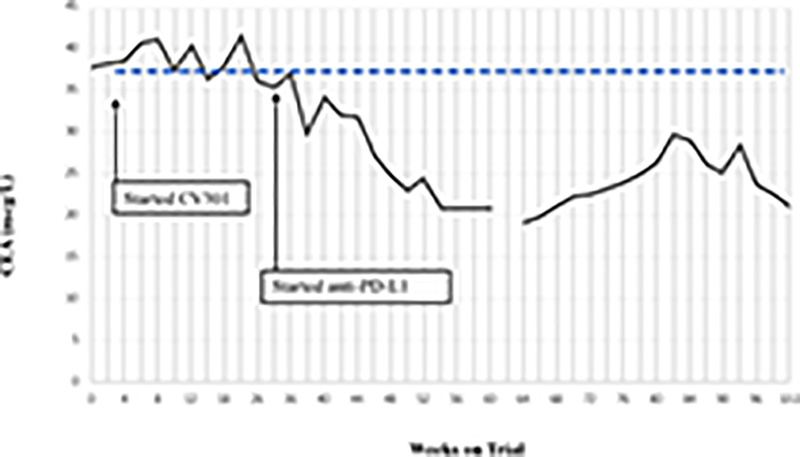
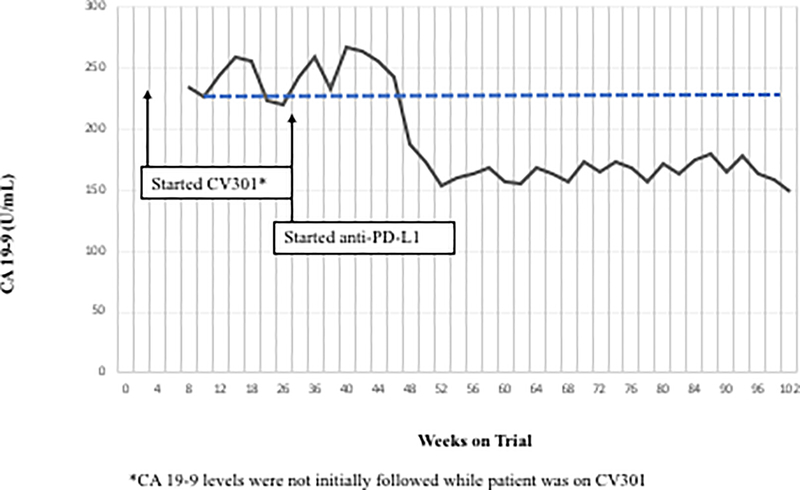
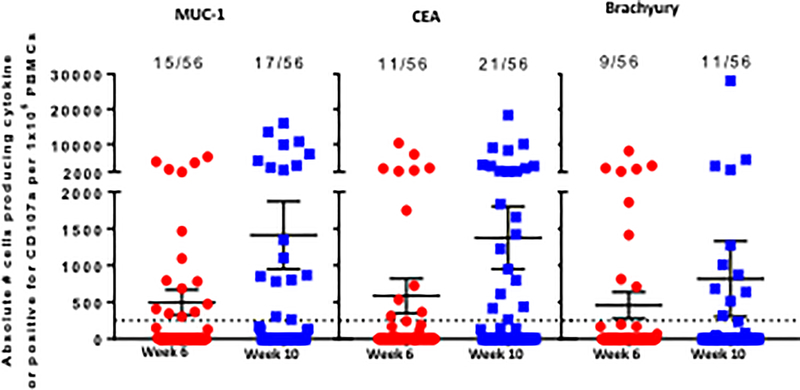
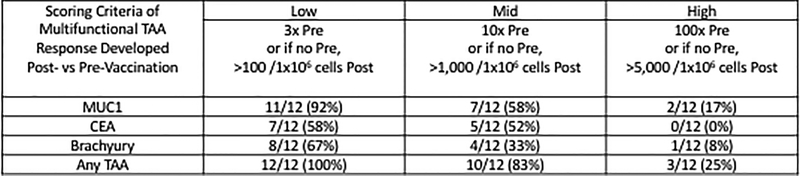
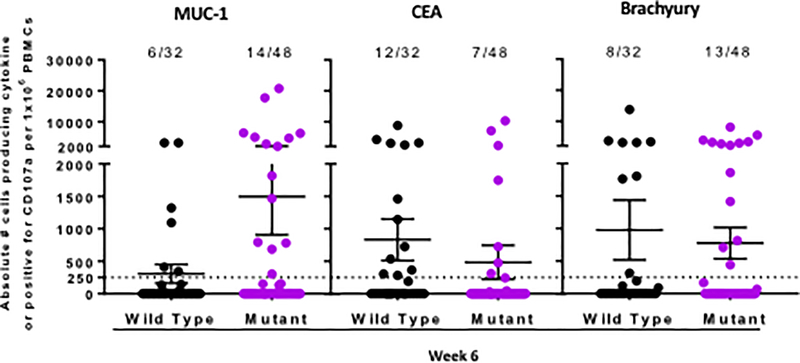
Results: There were no dose-limiting toxicities. Twelve patients enrolled on trial [dose level (DL) 1 = 3, DL2 = 3, DL3 = 6). Most side effects were seen with the prime doses and lessened with subsequent boosters. All treatment-related adverse events were temporary, self-limiting, grade 1/2, and included injection-site reactions and flu-like symptoms. Antigen-specific T cells to MUC1 and CEA, as well as to a cascade antigen, brachyury, were generated in most patients. Single-agent BN-CV301 produced a confirmed partial response (PR) in 1 patient and prolonged stable disease (SD) in multiple patients, most notably in KRAS-mutant gastrointestinal tumors. Furthermore, 2 patients with KRAS-mutant colorectal cancer had prolonged SD when treated with an anti-PD-L1 antibody following BN-CV301.
Conclusions: The BN-CV301 vaccine can be safely administered to patients with advanced cancer. Further studies of the vaccine in combination with other agents are planned.See related commentary by Repáraz et al., p. 4871.
©2019 American Association for Cancer Research.
Conflict of interest statement
Disclosure of Potential Conflicts of Interest:
M. Gatti-Mays, J. Strauss , R. Donahue, C. Palena, J. Del Rivero, J. Redman, R. Madan, J. Marté, L. Cordes, E. Lamping, J. Schlom and J. Gulley declare they have no potential conflicts to disclose. A. Orpia and A. Burmeister are employees of Leidos Biomedical Research. E. Wagner is an employee of Bavarian Nordic GmbH. C. Pico Navarro and C. Heery are employees of Bavarian Nordic.
Figures

Comment in
-
When Cancer Vaccines Go Viral.Clin Cancer Res. 2019 Aug 15;25(16):4871-4873. doi: 10.1158/1078-0432.CCR-19-1652. Epub 2019 Jun 21. Clin Cancer Res. 2019. PMID: 31227502
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
