

Patterns of survival in patients with recurrent mantle cell lymphoma in the modern era: progressive shortening in response duration and survival after each relapse
- PMID: 31110172
- PMCID: PMC6527702
- DOI: 10.1038/s41408-019-0209-5
Patterns of survival in patients with recurrent mantle cell lymphoma in the modern era: progressive shortening in response duration and survival after each relapse
Abstract
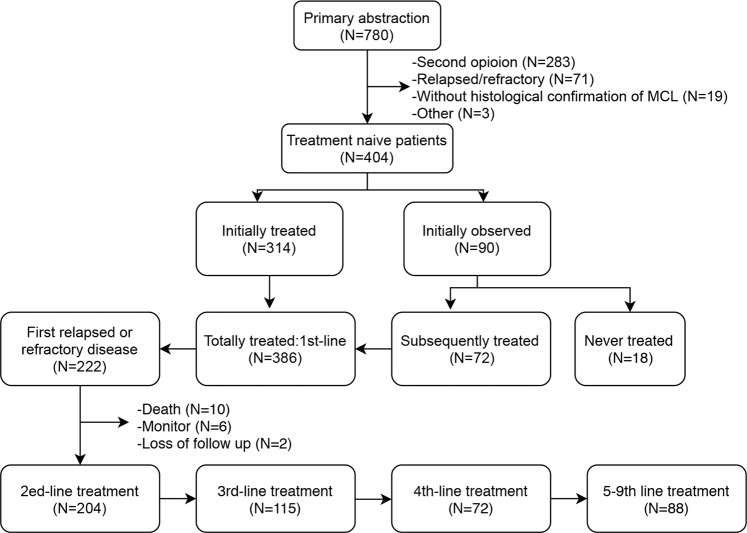
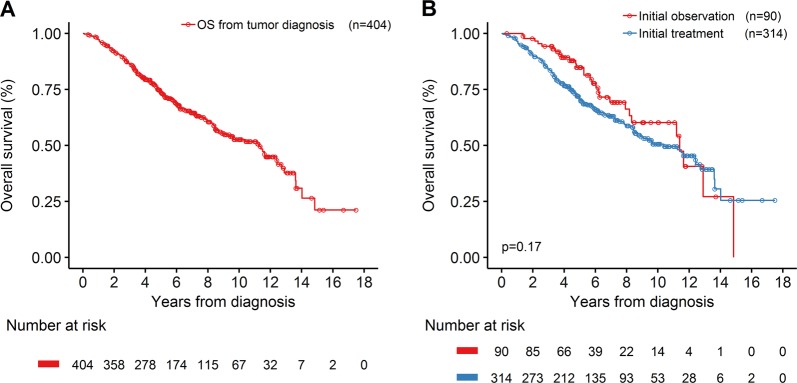
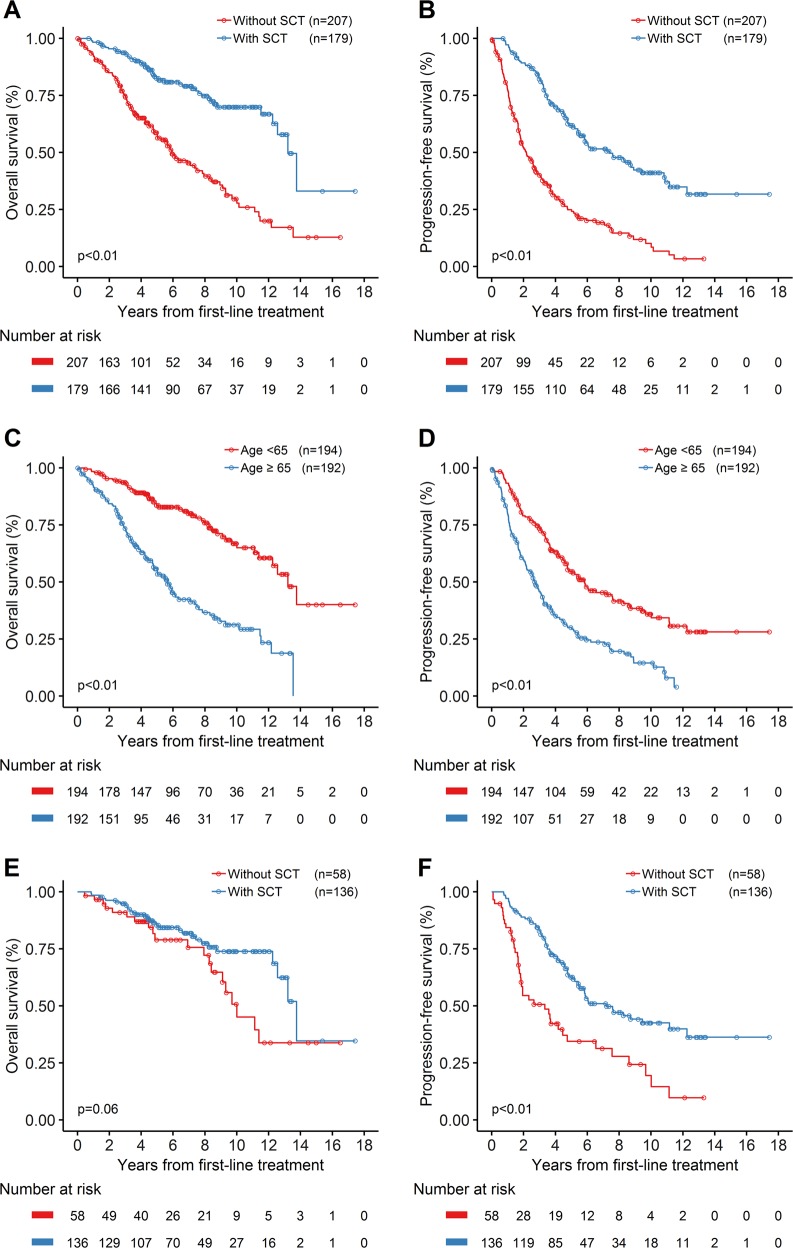
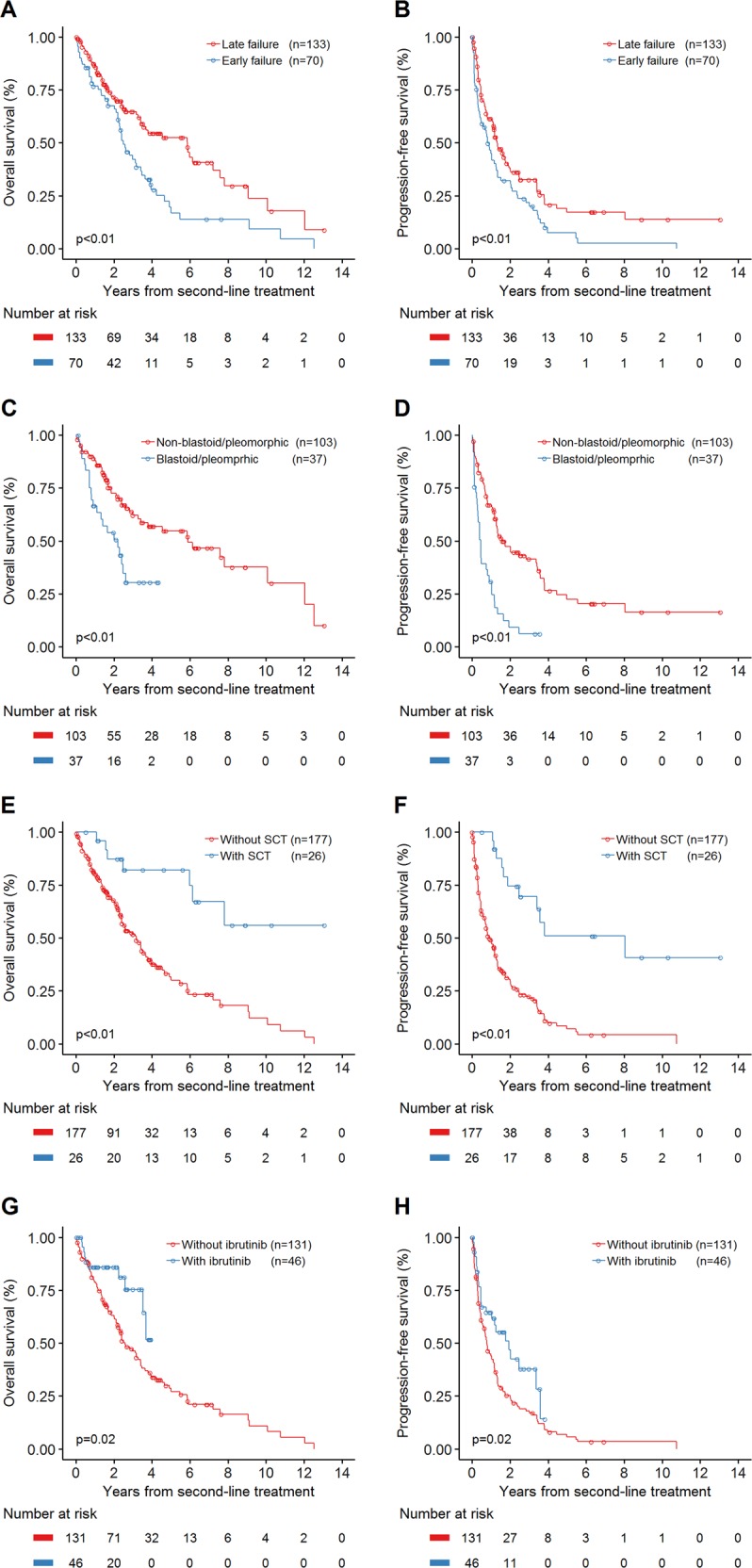
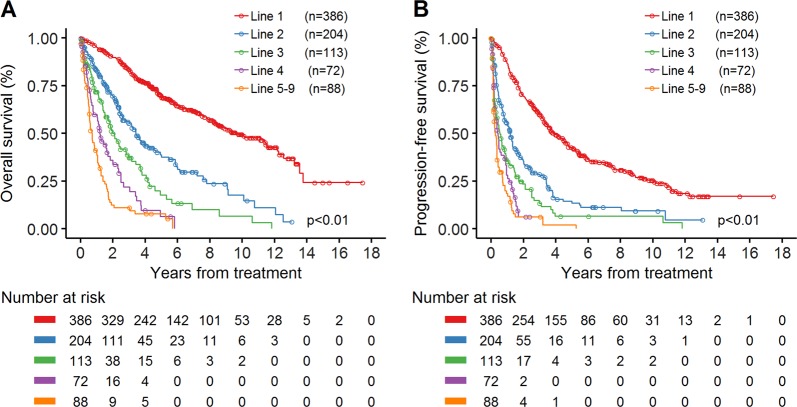
As the survival of patients with mantle cell lymphoma (MCL) continues to improve, patients are increasingly being treated with multiple regimens. However, outcome after each line remains poorly characterized in the modern era. To address this knowledge gap, we retrospectively studied 404 consecutive MCL patients who were managed between 2000 and 2014 at Memorial Sloan Kettering Cancer Center. Histologic diagnosis was centrally confirmed, and patients were followed longitudinally from diagnosis throughout their disease course. Progression-free survival (PFS) and overall survival (OS) were determined by Kaplan-Meier method. The median OS and PFS after first-line treatment were 9.7 and 4.0 years, respectively. After second-line therapy, the median OS and PFS were 41.1 and 14.0 months, third line were 25.2 and 6.5 months, and fourth line were 14.4 and 5.0 months. In patients less than 65 years, stem cell transplant (SCT)-based frontline regimens were associated with improved PFS compared with non-SCT regimens (median PFS: 86.2 versus 40.0 months; P < 0.01), with a trend toward longer OS (median OS: 165.0 versus 120.0 months; P = 0.06). Early treatment failure after first-line regimens was associated with worse OS (5.9 versus 2.5 years; P < 0.01). Our study should facilitate establishing proper endpoints for future clinical trials using novel treatment approaches.
Conflict of interest statement
A.K.: research funding from Abbvie Pharmaceuticals, Adaptive Biotechnologies, Celgene, Pharmacyclics, Seattle Genetics; advisory board member for Celgene (April 2016). F.S.: none. A.T.: none. A.D.: consultancy at Novartis, Weill-Cornell Hospital, Celgene, Seattle Genetics, Guidepoint Global Advisors, Pharmacyclics, Oncology Specialty Group, Roche, Peerview Institute, Physicians’ Education Resource, Corvus Pharmaceuticals. A.N.: none. C.L.B.: advisory for GLG, Defined Health; research funding from Novartis, Janssen, Bristol–Myers Squib, Epizyme, MedImmune; honoraria from Dava Oncology. M.L.M.P.: honoraria from Merck, Celgene and Pharmacyclics. C.P.: none. D.J.S.: consultancy at InPractice Elselvier, Seattle Genetics, Onco tracker (2016), Millenium (Takeda), DAVA (2016 and 2017), JUNO (2017), Bayer (2017); speaker’s bureau at ROCH China (2016), Medical Crossfire (2018). A.N.: research funding from Pharmacyclics, NIH, Raphael Pharma; consulting for: Janssen, Pharmacyclics, Medscape, Targeted Oncology. S.M.H.: consultancy at ADCT therapeutics, Aileron, Corvus, Forty-Seven, Innate Pharma, Kyowa-Hakka-Kirin, Millenium/Takeda, Mundipharma, Portola, Seattle Genetics; research funding from ADCT therapeutics, Aileron,Celgene, Forty-Seven, Infinity/Verastem, Kyowa-Hakka-Kirin, Millenium/Takeda, Seattle Genetics, Trillium. A.M.: consultancy at Kyowa Hakko Kirin Pharma, Miragen Therapeutics, Takeda Pharmaceuticals, ADC therapeutics, Seattle Genetics, Cell Medica, Bristol–Myers Squibb, Erytech Pharma; research funding from Incyte, Seattle Genetics, BMS, and Merck. P.H.: consultancy at Portola Pharmaceutics, Celgene, Karyopharm, Juno Therapeutics; research funding from Portola, Molecular Templates, Incyte, J&J Pharmaceuticals. C.H.M.: research funding from Merck, Seattle Genetics, BMS, ADC therapeutics Scientific Advisory Board: Novartis, Seattle Genetics, Takeda, Merck, BMS, Genentech, Astra Zeneca. M.J.M.: research funding from Genentech, Roche, GSK, Spectrum, Pharmacyclics, Seattle Genetics, Janssen; honoraria from Genentech, Roche, Spectrum, Janssen, Seattle Genetics, Rocket. A.D.Z.: consultancy at Genentech/Roche, Gilead, Celgene, Janssen, Amgen, Novartis, Adaptive Biotechnology; research funding MEI Pharma, MorphoSys, Sandoz, Celgene, Roche, Gilead; Board of Directors (DMC Chair) Beigene. A.Y.: research funding from Janssen, Novartis, Curis, Roche, BMS; honoraria or consulting fees from Bayer, Roche, BMS, Celgene, Incyte, Janssen, Curis, Takeda Millenium, Genentect, Merck, Xynomics, Bio-Path, and Epizyme.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
