

Intraoperative photoacoustic screening of breast cancer: a new perspective on malignancy visualization and surgical guidance
- PMID: 31111698
- PMCID: PMC6993064
- DOI: 10.1117/1.JBO.24.5.056002
Intraoperative photoacoustic screening of breast cancer: a new perspective on malignancy visualization and surgical guidance
Abstract
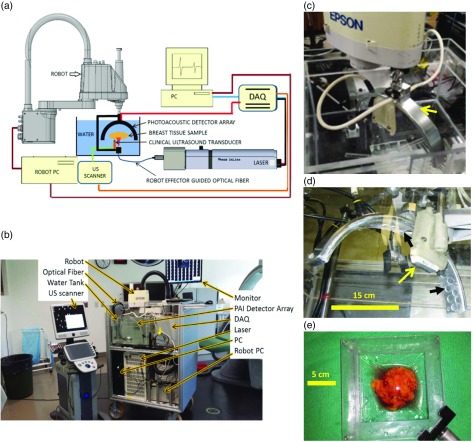
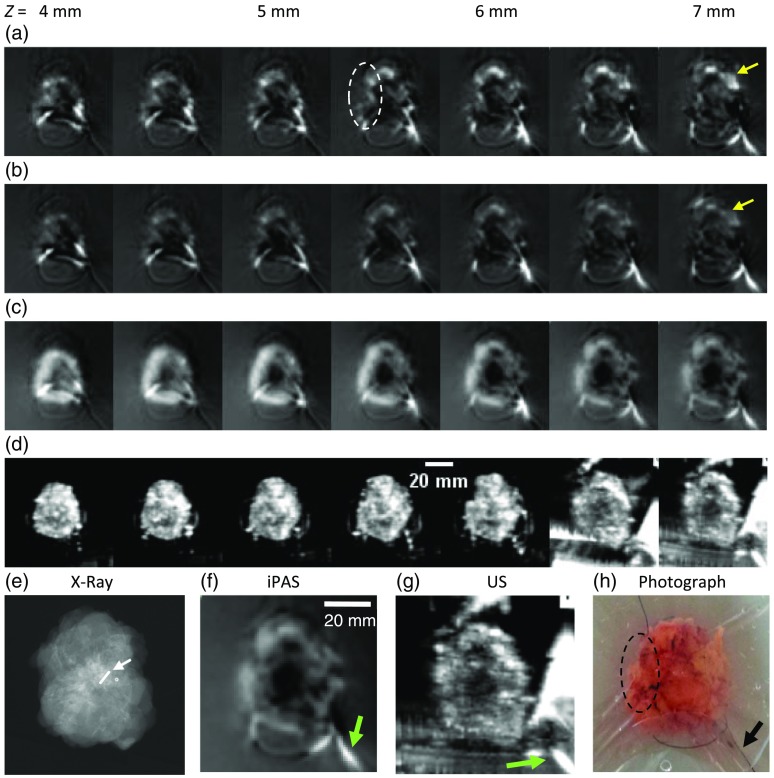
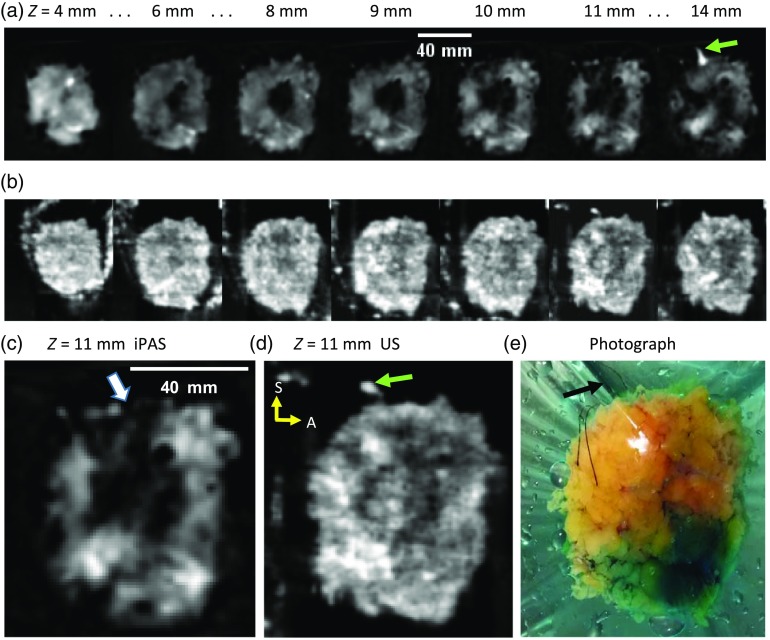
High re-excision rates in breast-conserving surgery call for a new intraoperative approach to the lumpectomy margin evaluation problem. The unique intraoperative imaging system, presented here, demonstrated the capability of photoacoustic tomography (PAT) to deliver optical sensitivity and specificity, along with over 2-cm imaging depth, in a clinical setting. The system enabled the evaluation of tumor extent, shape, morphology, and position within lumpectomy specimens measuring up to 11 cm in diameter. The investigation included all major breast cancer-related lesions, such as invasive ductal carcinoma (IDC), multifocal IDC, ductal carcinoma in situ and combinations of these variants. Coregistration with established ultrasound (US) technology, as well as comparison to specimen radiography, validated the performance of PAT, which appeared to facilitate better tumor visualization. Contrary to expected PA contrast mechanisms, PAT images of hemoglobin distribution correlated poorly with US-determined tumor location, while hypointense regions in lipid-weighted PAT images were in better agreement with US.
Keywords: breast cancer; photoacoustic; surgical guidance; three-dimensional; tomography.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
