

Interventions for the prevention of pain associated with the placement of intrauterine contraceptives: An updated review
- PMID: 31112295
- PMCID: PMC6900125
- DOI: 10.1111/aogs.13662
Interventions for the prevention of pain associated with the placement of intrauterine contraceptives: An updated review
Abstract
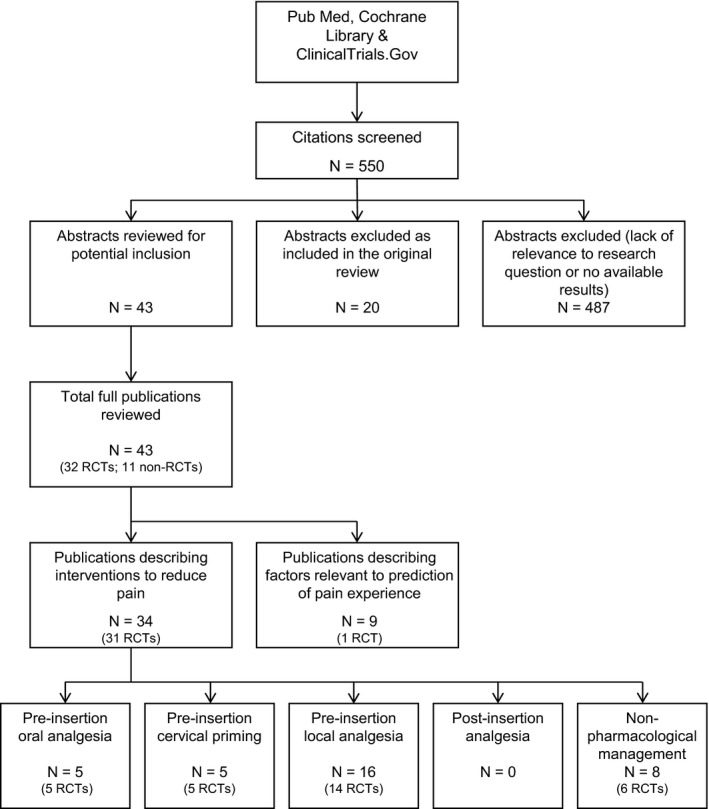
A 2013 review found no evidence to support the routine use of pain relief for intrauterine contraceptive (IUC) placement; however, fear of pain with placement continues to be a barrier to use for some women. This narrative review set out to identify (1) new evidence that may support routine use of pain management strategies for IUC placement; (2) procedure-related approaches that may have a positive impact on the pain experience; and (3) factors that may help healthcare professionals identify women at increased risk of pain with IUC placement. A literature search of the PubMed and Cochrane library databases revealed 550 citations, from which we identified 43 new and pertinent studies for review. Thirteen randomized clinical trials, published since 2012, described reductions in placement-related pain with administration of oral and local analgesia (oral ketorolac, local analgesia with different lidocaine formulations) and cervical priming when compared with placebo or controls. Four studies suggested that ultrasound guidance, balloon dilation, and a modified placement device may help to minimize the pain experienced with IUC placement. Eight publications suggested that previous cesarean delivery, timing of insertion relative to menstruation, dysmenorrhea, expected pain, baseline anxiety, and size of insertion tube may affect the pain experienced with IUC placement. Oral and local analgesia and cervical priming can be effective in minimizing IUC placement-related pain when compared with placebo, but routine use remains subject for debate. Predictive factors may help healthcare professionals to identify women at risk of experiencing pain. Targeted use of effective strategies in these women may be a useful approach while research continues in this area.
Keywords: contraception; intrauterine contraception; intrauterine device; nonsteroidal anti-inflammatory drugs; pain; women.
© 2019 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology(NFOG).
Conflict of interest statement
This publication and its content are solely the responsibility of the authors. KGD has participated in advisory board meetings on contraception and been the PI of clinical trials on IUS and other contraceptives, received honorarium for presentations on contraception for Bayer AG, MSD/Merck, HRA‐Pharma, Exeltis, Natural Cycles, and Mithra. These potential conflicts of interest have been reviewed and managed by KI. AdSS has participated as a member of Advisory Boards for Bayer AG. JTJ has received payments for consulting and research support from Bayer AG, Abbvie, Merck, HRA Pharma, Sebela, and the Population Council; consulting only from Cooper Surgical; and research support only from Daré, Mithra, and Medicines360. These companies and organizations may have a commercial or financial interest in the results of this research and technology. These potential conflicts of interest have been reviewed and managed by OHSU. TP has participated in Advisory Boards for Bayer AG and Shionogi Ltd. She has given presentations on Intrauterine Contraception and counseling and is a member of the INTRA Group. LB participated in advisory board meetings on contraception for Bayer AG and for MSD/Merck. IM and MR have nothing to disclose.
Figures
References
-
- Brockmeyer A, Kishen M, Webb A. Experience of IUD/IUS insertions and clinical performance in nulliparous women – a pilot study. Eur J Contracept Reprod Health Care. 2008;13:248‐254. - PubMed
-
- Marions L, Lövkvist L, Taube A, Johansson M, Dalvik H, Øverlie I. Use of the levonorgestrel‐releasing‐intrauterine system in nulliparous women – a non‐interventional study in Sweden. Eur J Contracept Reprod Health Care. 2011;16:126‐134. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
