

Candidaemia and a risk predictive model for overall mortality: a prospective multicentre study
- PMID: 31113382
- PMCID: PMC6528341
- DOI: 10.1186/s12879-019-4065-5
Candidaemia and a risk predictive model for overall mortality: a prospective multicentre study
Abstract
Background: Candidaemia is associated with high mortality. Variables associated with mortality have been published previously, but not developed into a risk predictive model for mortality. We sought to describe the current epidemiology of candidaemia in Australia, analyse predictors of 30-day all-cause mortality, and develop and validate a mortality risk predictive model.
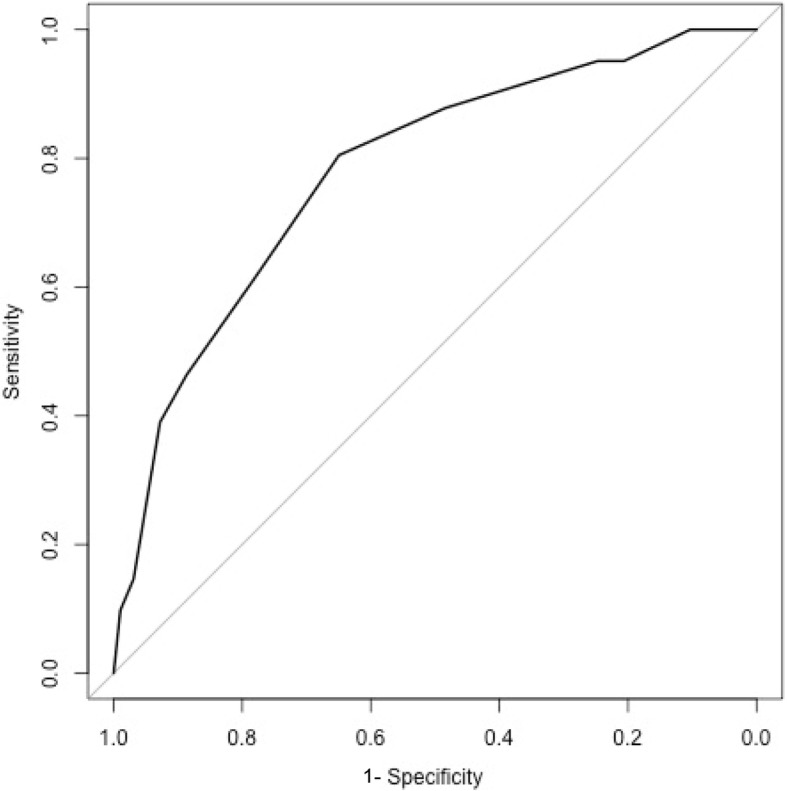
Methods: Adults with candidaemia were studied prospectively over 12 months at eight institutions. Clinical and laboratory variables at time of blood culture-positivity were subject to multivariate analysis for association with 30-day all-cause mortality. A predictive score for mortality was examined by area under receiver operator characteristic curves and a historical data set was used for validation.
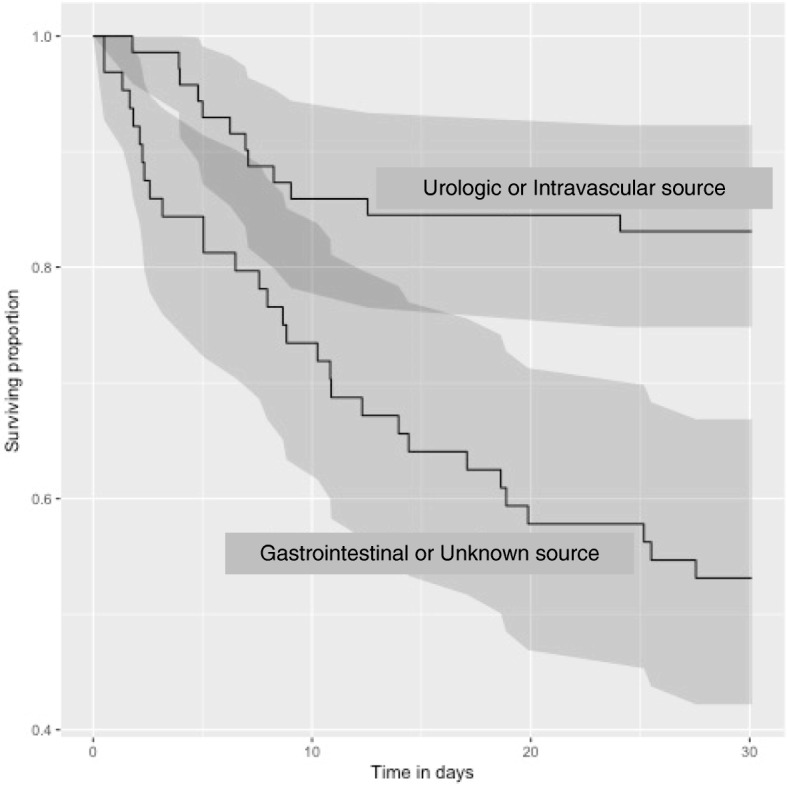
Results: The median age of 133 patients with candidaemia was 62 years; 76 (57%) were male and 57 (43%) were female. Co-morbidities included underlying haematologic malignancy (n = 20; 15%), and solid organ malignancy in (n = 25; 19%); 55 (41%) were in an intensive care unit (ICU). Non-albicans Candida spp. accounted for 61% of cases (81/133). All-cause 30-day mortality was 31%. A gastrointestinal or unknown source was associated with higher overall mortality than an intravascular or urologic source (p < 0.01). A risk predictive score based on age > 65 years, ICU admission, chronic organ dysfunction, preceding surgery within 30 days, haematological malignancy, source of candidaemia and antibiotic therapy for ≥10 days stratified patients into < 20% or ≥ 20% predicted mortality. The model retained accuracy when validated against a historical dataset (n = 741).
Conclusions: Mortality in patients with candidaemia remains high. A simple mortality risk predictive score stratifying patients with candidaemia into < 20% and ≥ 20% 30-day mortality is presented. This model uses information available at time of candidaemia diagnosis is easy to incorporate into decision support systems. Further validation of this model is warranted.
Keywords: Candida blood stream infection; Candidaemia; Invasive fungal infection; Mortality; Risk stratification score.
Conflict of interest statement
SC, MS, SVH and DM are on the Antifungal Advisory Boards of Gilead Sciences Inc., MSD Australia and Pfizer Australia. SK is on the Antifungal Advisory Board of Pfizer Australia, MSD Australia and Mayne Pharma. TS, DM, MS, SC, SVH, NB, CK and SK have received untied grants from Gilead Sciences Inc., MSD Australia and Pfizer Australia. All other authors: none to declare.
Figures
References
-
- Lockhart SR, Iqbal N, Cleveland AA, Farley MM, Harrison LH, Bolden CB, et al. Species identification and antifungal susceptibility testing of Candida bloodstream isolates from population-based surveillance studies in two U.S. cities from 2008 to 2011. J Clin Microbiol. 2012;50(11):3435–3442. doi: 10.1128/JCM.01283-12. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
