

CARMIL2 Deficiency Presenting as Very Early Onset Inflammatory Bowel Disease
- PMID: 31115454
- PMCID: PMC6799948
- DOI: 10.1093/ibd/izz103
CARMIL2 Deficiency Presenting as Very Early Onset Inflammatory Bowel Disease
Abstract
Background: Children with very early onset inflammatory bowel diseases (VEO-IBD) often have a refractory and severe disease course. A significant number of described VEO-IBD-causing monogenic disorders can be attributed to defects in immune-related genes. The diagnosis of the underlying primary immunodeficiency (PID) often has critical implications for the treatment of patients with IBD-like phenotypes.
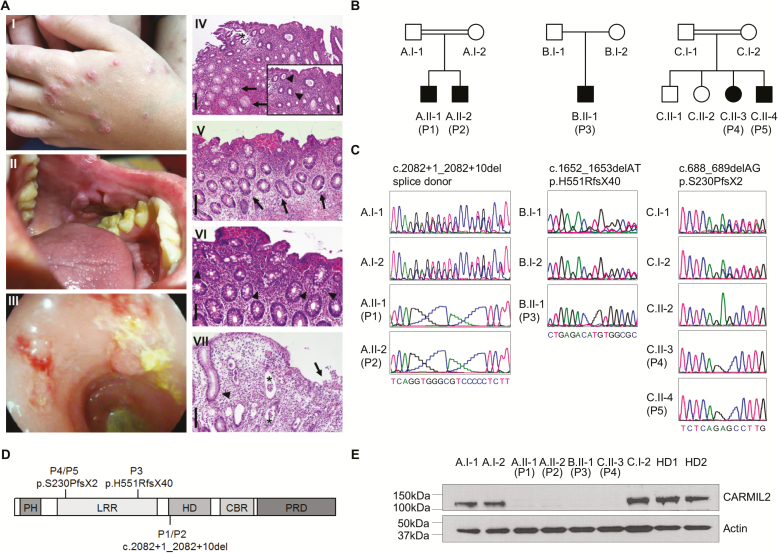
Methods: To identify the molecular etiology in 5 patients from 3 unrelated kindred with IBD-like symptoms, we conducted whole exome sequencing. Immune workup confirmed an underlying PID.
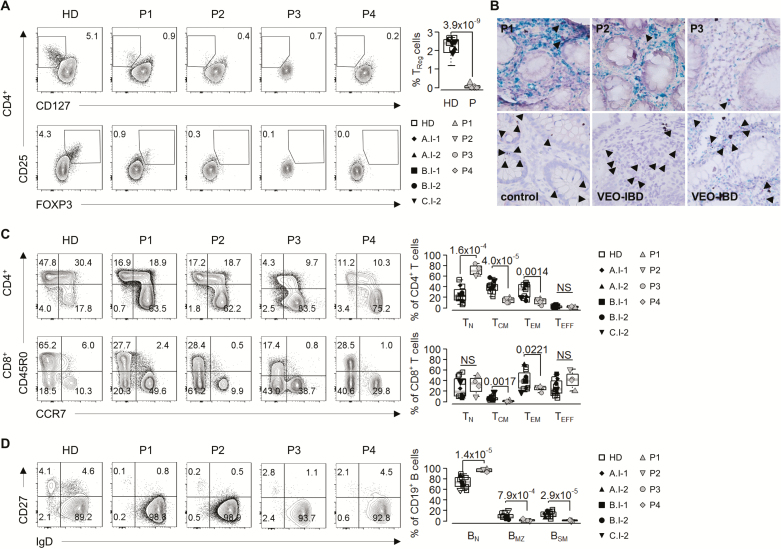
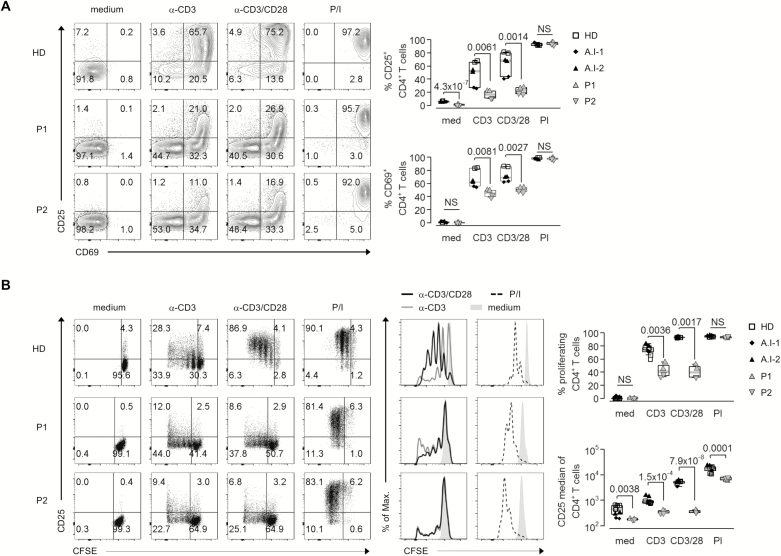
Results: Whole exome sequencing revealed 3 novel CARMIL2 loss-of-function mutations in our patients. Immunophenotyping of peripheral blood mononuclear cells showed reduction of regulatory and effector memory T cells and impaired B cell class switching. The T cell proliferation and activation assays confirmed defective responses to CD28 costimulation, consistent with CARMIL2 deficiency.
Conclusion: Our study highlights that human CARMIL2 deficiency can manifest with IBD-like symptoms. This example illustrates that early diagnosis of underlying PID is crucial for the treatment and prognosis of children with VEO-IBD.
Keywords: CARMIL2; immunodeficiency; very early onset inflammatory bowel diseases.
© 2019 Crohn’s & Colitis Foundation. Published by Oxford University Press. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Uhlig HH. Monogenic diseases associated with intestinal inflammation: implications for the understanding of inflammatory bowel disease. Gut. 2013;62:1795–1805. - PubMed
-
- Fischer A. Human primary immunodeficiency diseases: a perspective. Nat Immunol. 2004;5:23–30. - PubMed
-
- Pachlopnik Schmid J, Canioni D, Moshous D, et al. . Clinical similarities and differences of patients with X-linked lymphoproliferative syndrome type 1 (XLP-1/SAP deficiency) versus type 2 (XLP-2/XIAP deficiency). Blood. 2011;117:1522–1529. - PubMed
