

An update on Burkitt lymphoma: a review of pathogenesis and multimodality imaging assessment of disease presentation, treatment response, and recurrence
- PMID: 31115699
- PMCID: PMC6529494
- DOI: 10.1186/s13244-019-0733-7
An update on Burkitt lymphoma: a review of pathogenesis and multimodality imaging assessment of disease presentation, treatment response, and recurrence
Abstract
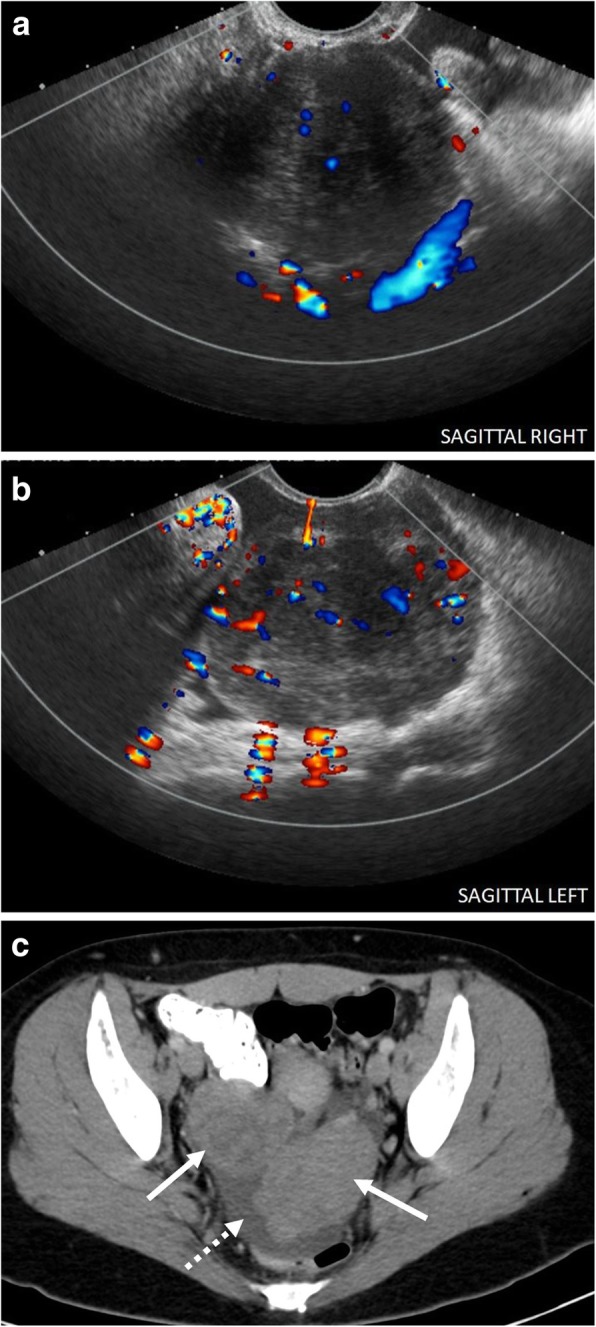
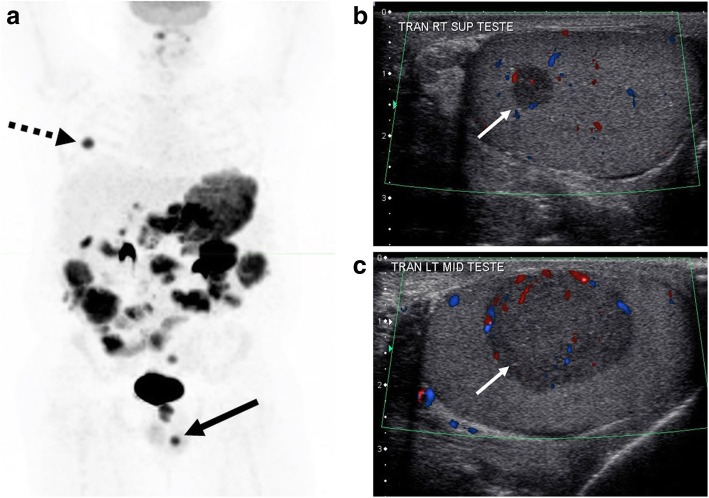
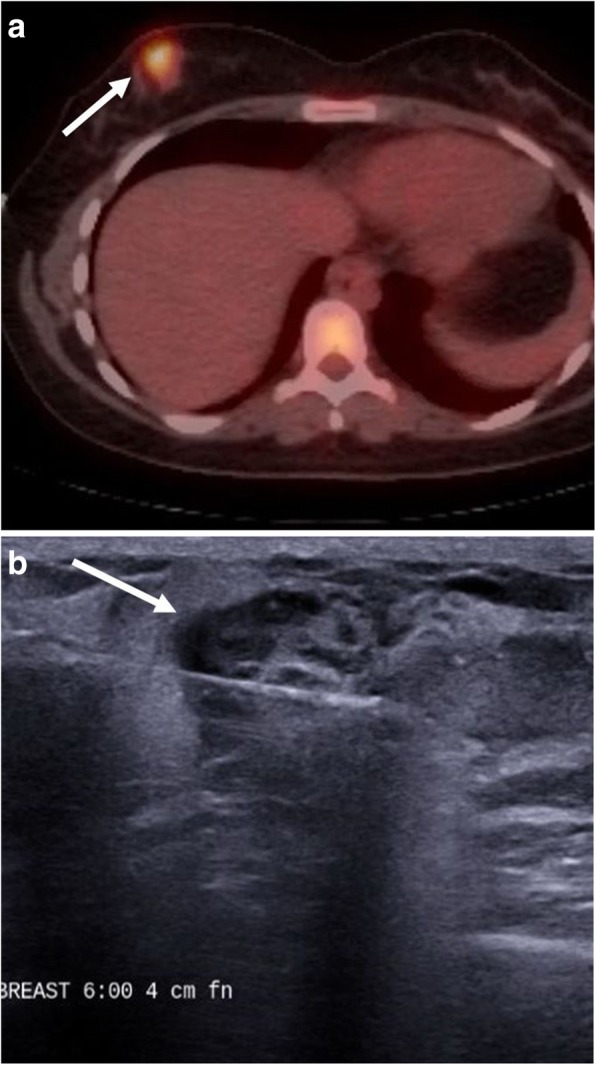
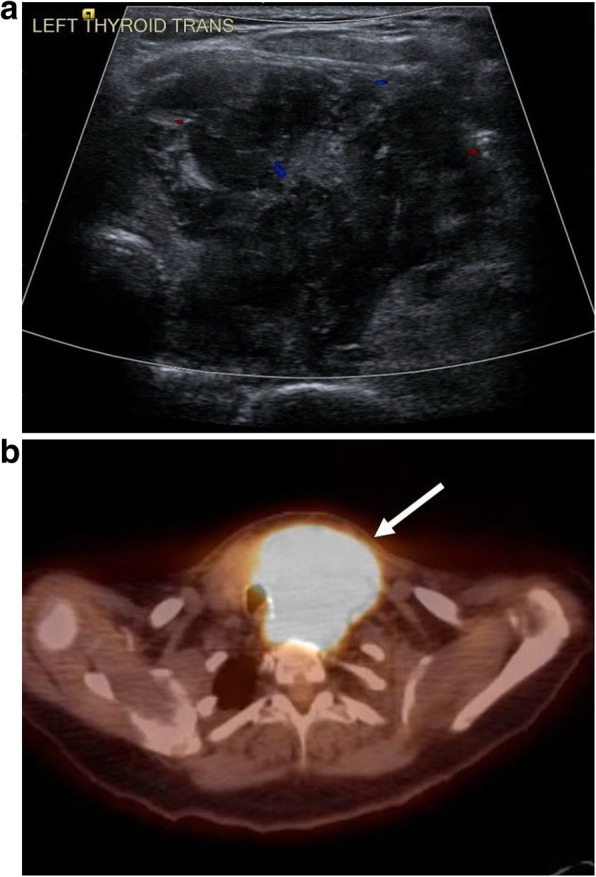
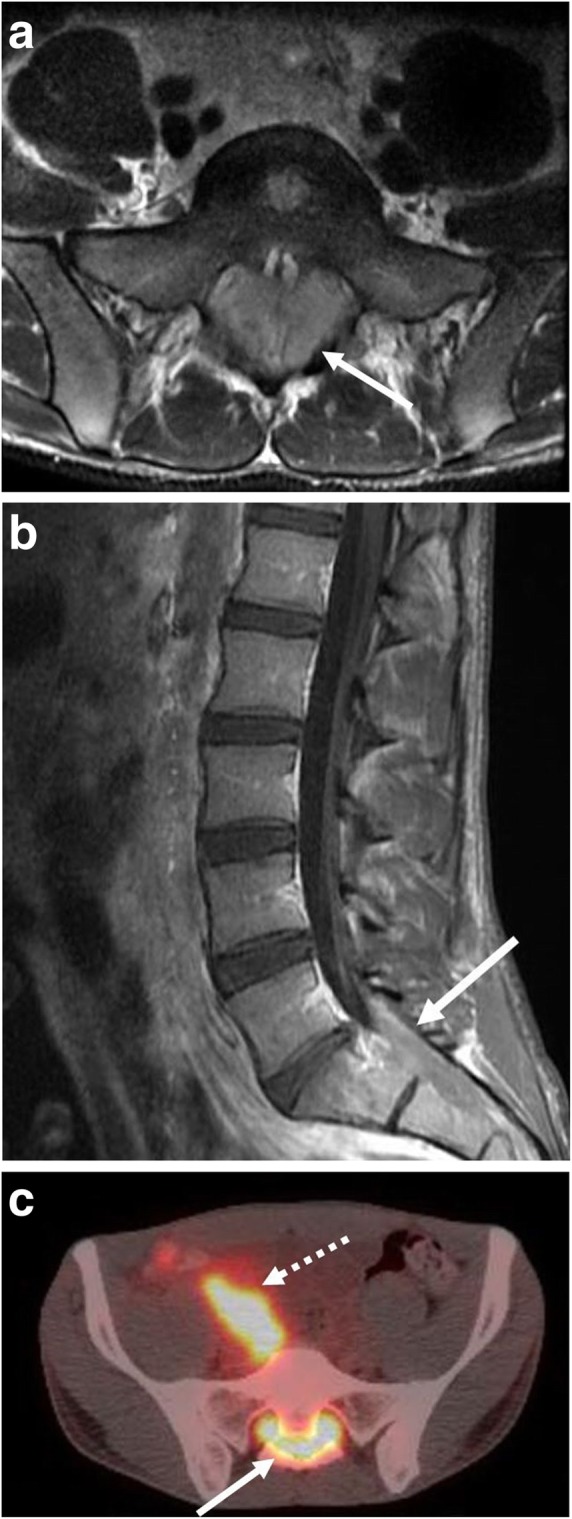
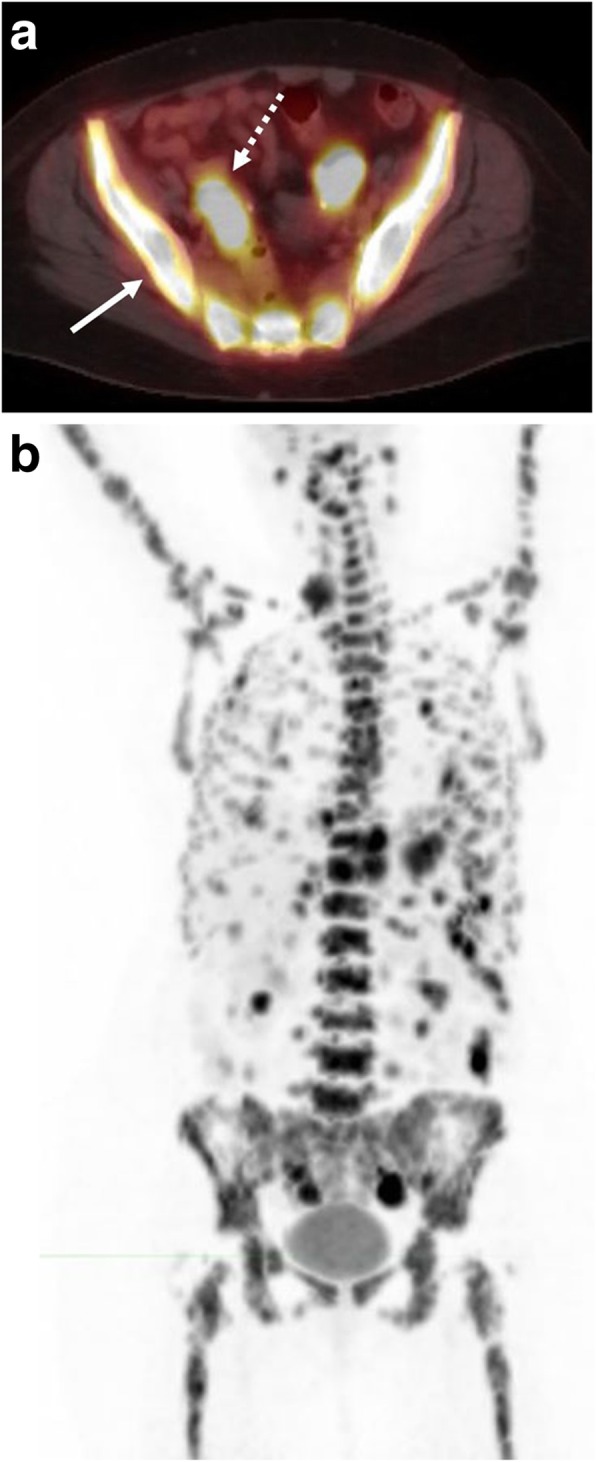
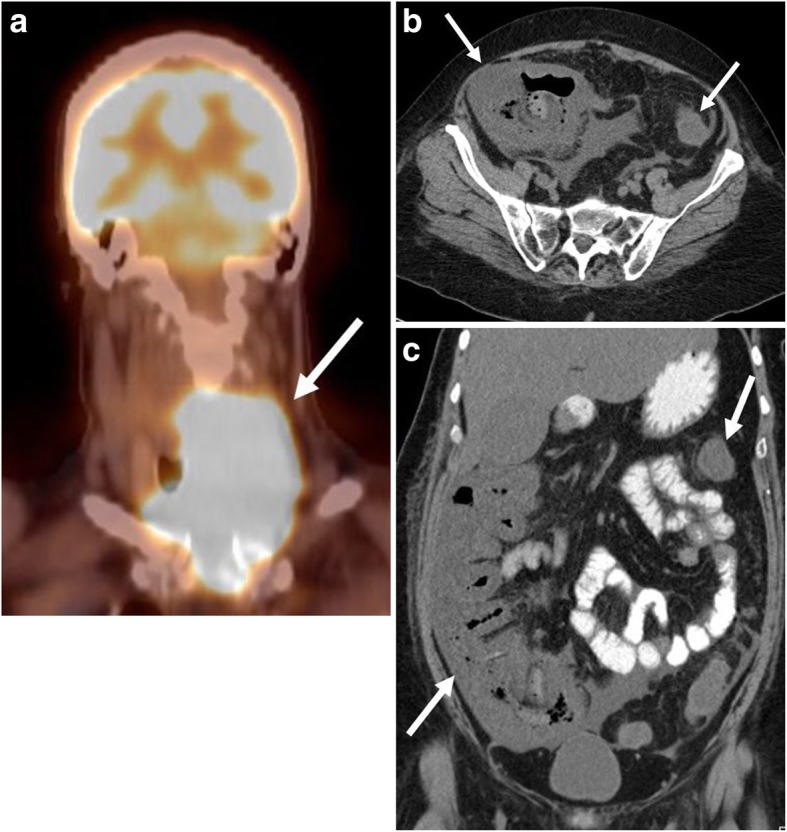
Burkitt lymphoma (BL) is a highly aggressive, rapidly growing B cell non-Hodgkin lymphoma, which manifests in several subtypes including sporadic, endemic, and immunodeficiency-associated forms. Pathologically, BL is classically characterized by translocations of chromosomes 8 and 14 resulting in upregulation of the c-myc protein transcription factor with upregulation of cell proliferation. BL affects nearly every organ system, most commonly the abdomen and pelvis in the sporadic form. Imaging using a multimodality approach plays a crucial role in the management of BL from diagnosis, staging, and evaluation of treatment response to therapy-related complications with ultrasound, computed tomography, magnetic resonance imaging, and positron emission tomography playing roles. In this article, we review the pathobiology and classification of BL, illustrate a multimodality imaging approach in evaluating common and uncommon sites of involvement within the trunk and head and neck, and review common therapies and treatment-related complications.
Keywords: B cell; Burkitt lymphoma; Computed tomography; Diagnostic imaging; Drug therapy; Lymphoma.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures





References
Publication types
LinkOut - more resources
Full Text Sources
