

Formyl peptide receptor 1 up-regulation and formyl peptide receptor 2/3 down-regulation of blood immune cells along with defective lipoxin A4/resolvin D1 production in obstructive sleep apnea patients
- PMID: 31116781
- PMCID: PMC6530856
- DOI: 10.1371/journal.pone.0216607
Formyl peptide receptor 1 up-regulation and formyl peptide receptor 2/3 down-regulation of blood immune cells along with defective lipoxin A4/resolvin D1 production in obstructive sleep apnea patients
Abstract
Background: This study aims to investigate the role of FPR 1/2/3 expressions in patients with obstructive sleep apnea (OSA).
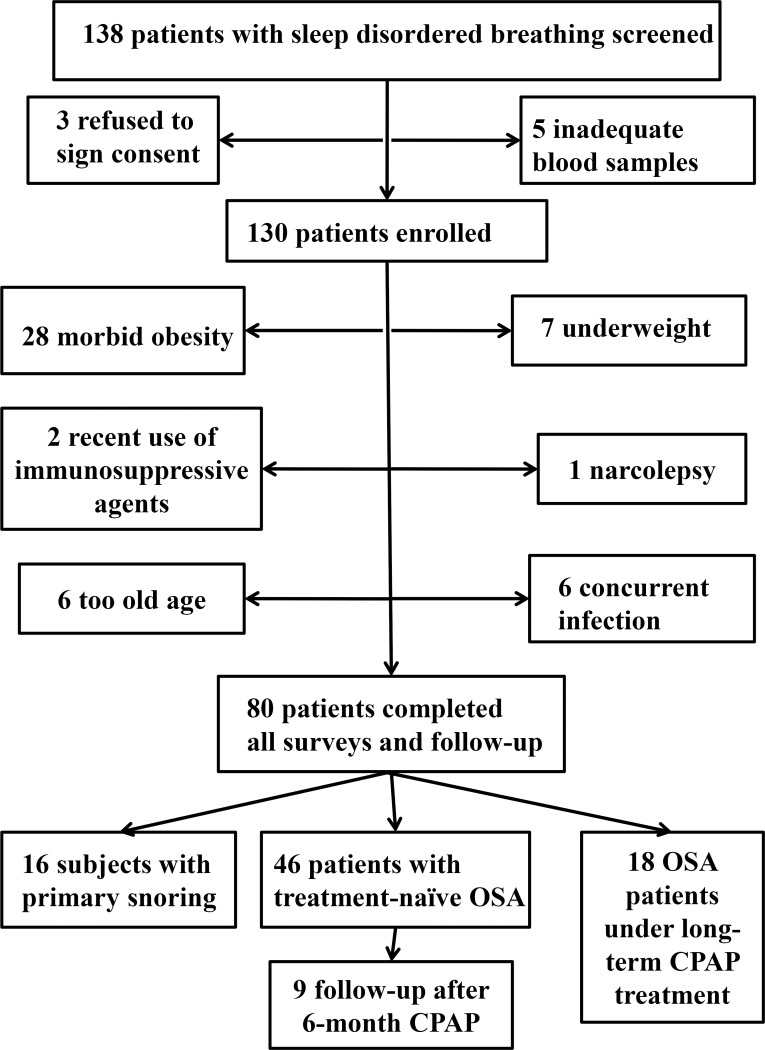
Method: We made cross-sectional comparisons of FPR1/2/3 expressions of blood neutrophil, M1/M2a monocyte, and natural killer (NK) cell between 16 healthy subjects (HS), 16 primary snoring (PS) subjects, 46 treatment-naive OSA patients, and 18 severe OSA patients under long-term continuous positive airway pressure treatment (severe OSA on CPAP).
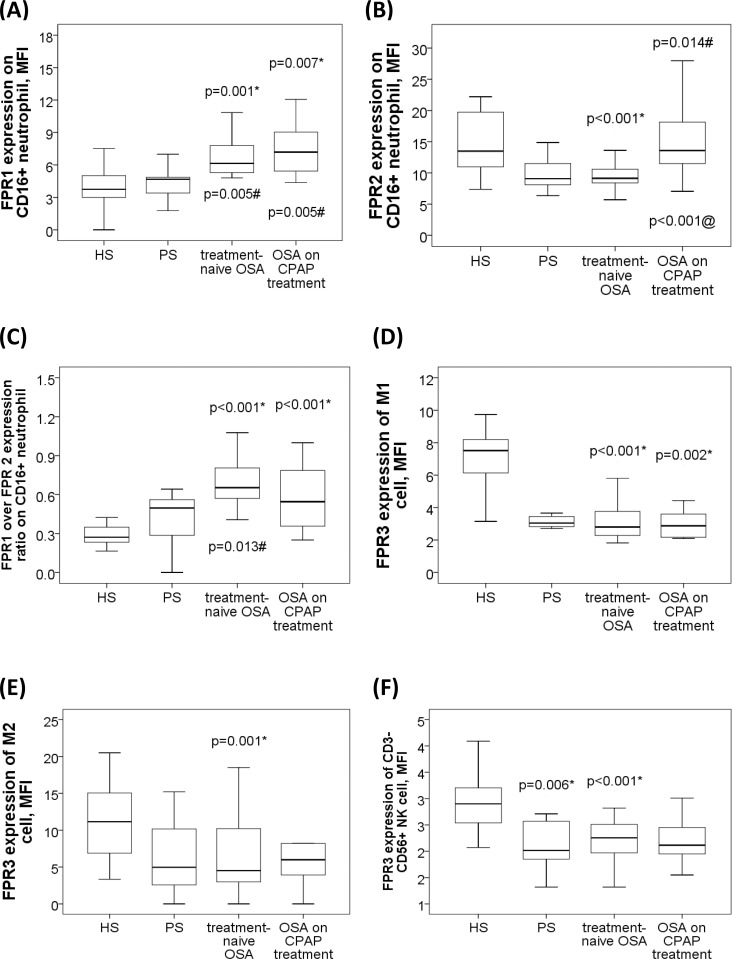
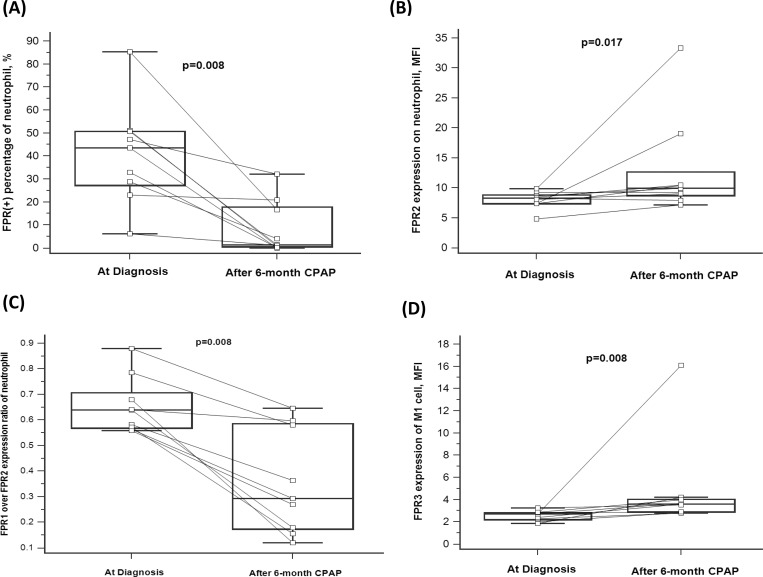
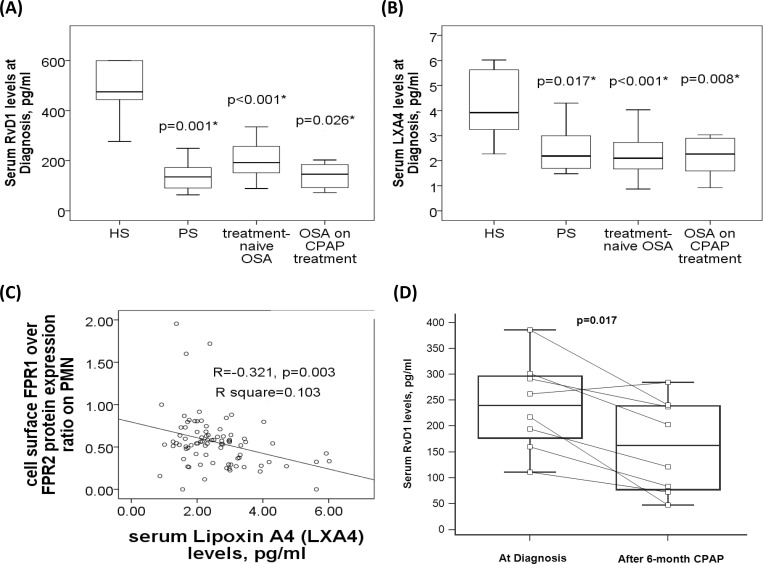
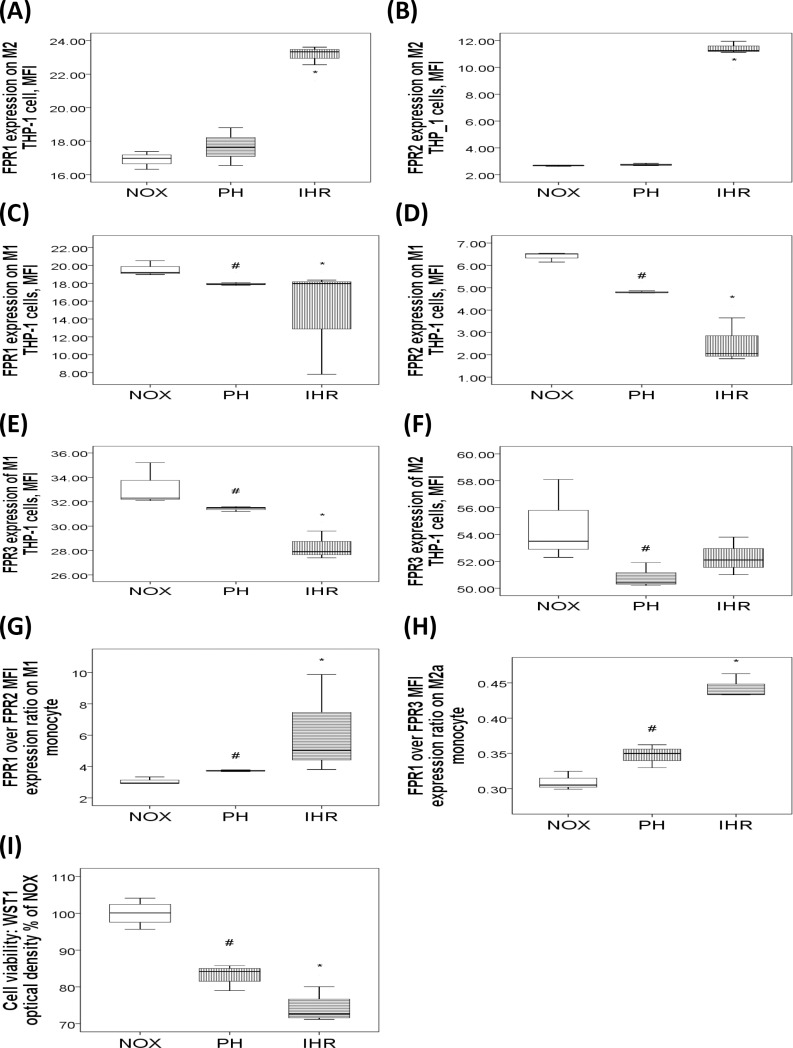
Results: FPR1 expressions on neutrophil were increased in treatment-naive OSA and severe OSA on CPAP groups versus either HS or PS. FPR2 expressions on neutrophil were decreased in treatment-naive OSA versus HS, and returned to normal in severe OSA on CPAP group. FPR1/FPR2 expression ratio on neutrophil was increased in treatment-naive OSA versus either HS or PS. Serum lipoxin A4, resolvin D1 levels, and FPR3 expressions of M1, M2a and NK cells were all decreased in treatment-naive OSA versus HS. OSA patients with hypertension had decreased FPR2 expressions on neutrophil and FPR3 expressions of NK cell. FPR1 expression, FPR1/FPR2 expression ratio on neutrophil, and FPR3 expression of M1 cell were all reversed after > 6-month CPAP treatment in 9 selected patients. In vitro intermittent hypoxia with re-oxygenation treatment in THP-1 cells resulted in increased FPR1/FPR2 expression ratio of M1 cells, and increased FPR1/FPR3 expression ratio of M2a cells.
Conclusions: FPR1 over-expression and insufficiency of FPR2 and FPR3 in association with defective lipoxin A4 and resolving D1 production were associated with disease severity of OSA and its adverse consequences.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Siarnik P, Carnicka Z, Krizova L, Wagnerova H, Sutovsky S, Klobucnikova K, et al. Predictors of impaired endothelial function in obstructive sleep apnea syndrome. Neuro endocrinology letters. 2014;35(2):142–8. . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
