

It's more than low BMI: prevalence of cachexia and associated mortality in COPD
- PMID: 31118043
- PMCID: PMC6532157
- DOI: 10.1186/s12931-019-1073-3
It's more than low BMI: prevalence of cachexia and associated mortality in COPD
Abstract
Background: Cachexia is associated with increased mortality risk among chronic obstructive pulmonary disease (COPD) patients. However, low body mass index (BMI) as opposed to cachexia is often used, particularly when calculating the BODE (BMI, Obstruction, Dyspnea and Exercise) index. For this reason, we examined mortality using a consensus definition and a weight-loss definition of cachexia among COPD cases and compared two new COPD severity indices with BODE.
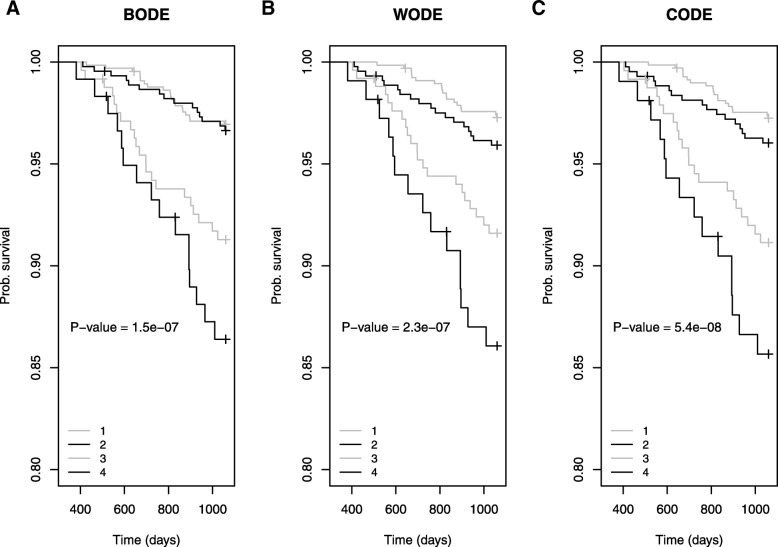
Methods: In the current report, the consensus definition for cachexia incorporated weight-loss > 5% in 12-months or low BMI in addition to 3/5 of decreased muscle strength, fatigue, anorexia, low FFMI and inflammation. The weight-loss definition incorporated weight-loss > 5% or weight-loss > 2% (if low BMI) in 12-months. The low BMI component in BODE was replaced with the consensus definition to create the CODE (Consensus cachexia, Obstruction, Dyspnea and Exercise) index and the weight-loss definition to create the WODE (Weight loss, Obstruction, Dyspnea and Exercise) index. Mortality was assessed using Kaplan-Meier survival and Cox Regression. Performance of models was compared using C-statistics.
Results: Among 1483 COPD cases, the prevalences of cachexia by the consensus and weight-loss definitions were 4.7 and 10.4%, respectively. Cachectic patients had a greater than three-fold increased mortality by either the consensus or the weight-loss definition of cachexia independent of BMI and lung function. The CODE index predicted mortality slightly more accurately than the BODE and WODE indices.
Conclusions: Cachexia is associated with increased mortality among COPD patients. Monitoring cachexia using weight-loss criteria is relatively simple and predictive of mortality among COPD cases who may be missed if only low BMI is used.
Keywords: BMI; BODE; COPD; Cachexia; Weight loss.
Conflict of interest statement
M-LNM reports grants from National Institutes of Health, other from Parker B. Francis Foundation, during the conduct of the study and personal fees from Pfizer, outside the submitted work.
EFMW has received personal fees from Nycomed, Boehringer, AstraZeneca, GSK, Novartis and Chiesi. EFMW has received grants from AstraZeneca and GSK.
ER has no competing interests.
RC has received personal fees from GSK, Boehringer Ingelheim, Astra Zeneca, Genentech and Regeneron.
SIR reports other from AstraZeneca, outside the submitted work. S.I.R. is employed by AstraZeneca.
DAL reports grants, personal fees and non-financial support from GSK during the conduct of the study and personal fees from Griffols, outside the submitted work.
MB has no competing interests.
BC reports personal fees and other from Astra Zeneca, personal fees from GlaxoSmithKline, personal fees from Boehringer Ingelheim, personal fees from Novartis, personal fees from Sanofi Aventis and personal fess form Menarini other from outside the submitted work.
AA reports personal fees from GSK, during the conduct of the study.
RT-S is an employee and shareholder of GSK, the ECLIPSE study sponsor.
CPH reports personal fees from Mylan, personal fees from AstraZeneca, personal fees from Concert Pharmaceuticals, personal fees from 23andMe, grants from Novartis, grants from Boehringer-Ingelheim, grants from NHLBI, outside the submitted work.
MD reports grants from Department of Defense, personal fees and other from Boehringer Ingelheim, personal fees and other from GSK, other from Novartis, personal fees and other from AstraZeneca, other from Yungjin, personal fees and other from PneumRx/BTG, other from Pulmonx, personal fees from Genentech, personal fees and other from Boston Scientific, personal fees from Quark Pharmaceuticals, grants from NIH, outside the submitted work.
EKS reports grants, personal fees and other from GSK, during the conduct of the study; personal fees from Novartis, outside the submitted work.
Figures



References
-
- Evans WJ, Morley JE, Argiles J, Bales C, Baracos V, Guttridge D, Jatoi A, Kalantar-Zadeh K, Lochs H, Mantovani G, Marks D, Mitch WE, Muscaritoli M, Najand A, Ponikowski P, Rossi Fanelli F, Schambelan M, Schols A, Schuster M, Thomas D, Wolfe R, Anker SD. Cachexia: a new definition. Clin Nutr. 2008;27:793–799. doi: 10.1016/j.clnu.2008.06.013. - DOI - PubMed
