

Neurologic toxicity associated with immune checkpoint inhibitors: a pharmacovigilance study
- PMID: 31118078
- PMCID: PMC6530194
- DOI: 10.1186/s40425-019-0617-x
Neurologic toxicity associated with immune checkpoint inhibitors: a pharmacovigilance study
Abstract
Background: Immune checkpoint inhibitors (ICI) produce durable antitumor responses but provoke autoimmune toxicities, including uncommon but potentially devastating neurologic toxicities. The clinical features, including the spectrum, timing, and outcomes, of ICI-induced neurologic toxicities are not well characterized.
Methods: We performed disproportionality analysis using Vigibase, the World Health Organization pharmacovigilance database, comparing neurologic adverse event (AE) reporting in patients receiving ICIs vs. the full database. Neurologic AEs were classified by group queries using Medical Dictionary for Regulatory Activities, between database inception to September 28, 2018. Associations between ICIs and neurologic AEs were assessed using reporting odds ratios (ROR) and information component (IC). IC compares observed and expected values to find associations between drugs and AEs using disproportionate Bayesian reporting; IC025 (lower end of the IC 95% credibility interval) > 0 is considered statistically significant.
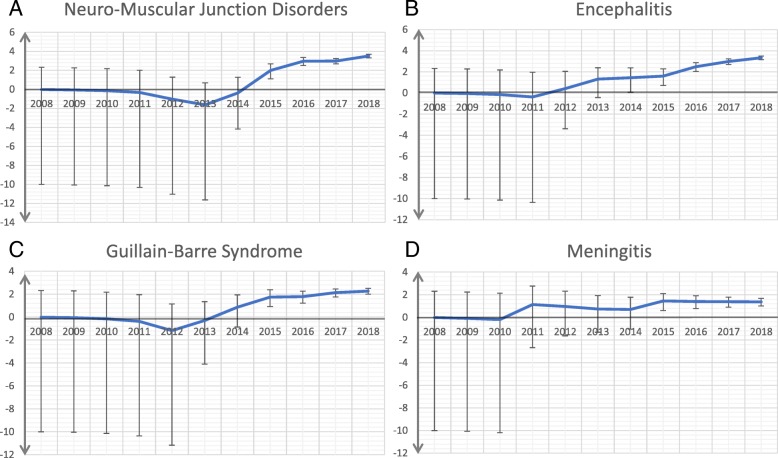
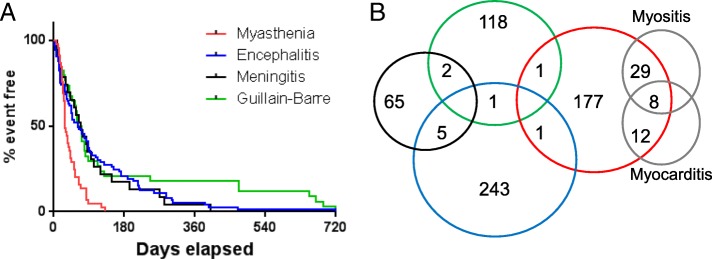
Results: Among the full database, 18,518,994 AEs were reported, including 48,653 with ICIs. ICIs were associated with higher incidence of myasthenia gravis (0.47% of ICI reports vs. 0.04% of the full database, ROR 16.5 [95% CI 14.5-18.9]; IC025 3.31), encephalitis (0.51% vs. 0.05%, ROR 10.4 [95% CI 9.2-11.8]; IC025 3.15), peripheral neuropathy (1.16% vs. 0.67%, IC025 0.68), and meningitis (0.15% vs. 0.06%, ROR 3.1 [95% CI 2.5-3.9]; IC025 1.01). Myasthenia gravis and encephalitis were associated with anti-PD-1 whereas other neurologic AEs were associated with anti-CTLA-4. Myasthenia gravis was characterized by high fatality rates (~ 20%), early onset (median 29 days), and frequent concurrent myocarditis and myositis; whereas other neurologic AEs had lower fatality rates (6-12%), later onset (median 61-80 days), and were non-overlapping.
Conclusions: ICIs produce a spectrum of distinct classes of neurologic AEs that can cause significant morbidity and mortality and tend to occur early and with class-specific associations.
Keywords: CTLA-4; Encephalitis; Guillain-Barre syndrome; Myasthenia gravis; Neuropathy; Neurotoxicity; PD-1; PD-L1.
Conflict of interest statement
DBJ serves on advisory boards for Array Biopharma, BMS, Genoptix, Incyte, and Merck, and receives research funding from BMS and Incyte. JJM serves on advisory boards for Pfizer, Novartis, BMS, Takeda, Myokardia, Regeneron, and Decipher, and receives research funding from BMS and Pfizer.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials