

Identification of Myocardial Disarray in Patients With Hypertrophic Cardiomyopathy and Ventricular Arrhythmias
- PMID: 31118142
- PMCID: PMC6548973
- DOI: 10.1016/j.jacc.2019.02.065
Identification of Myocardial Disarray in Patients With Hypertrophic Cardiomyopathy and Ventricular Arrhythmias
Abstract
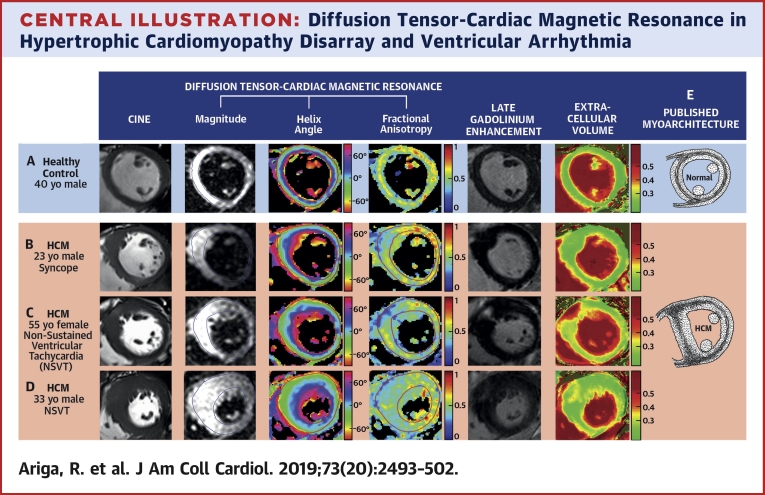
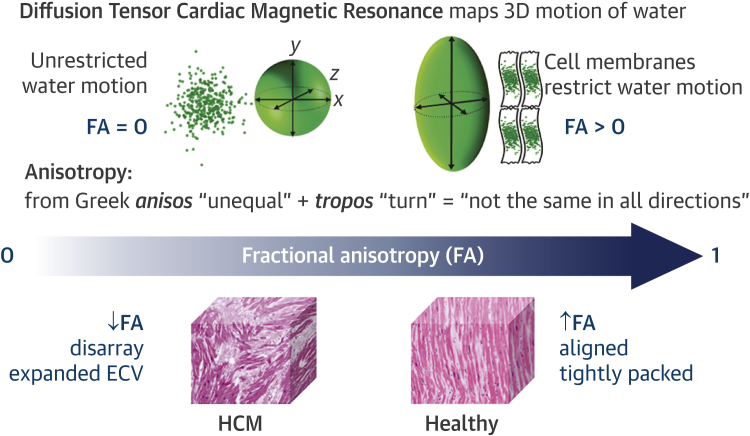
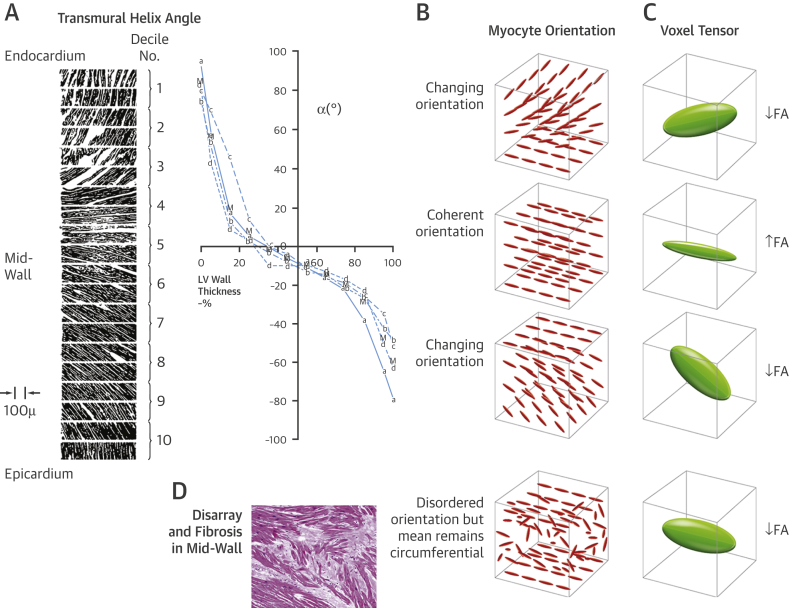
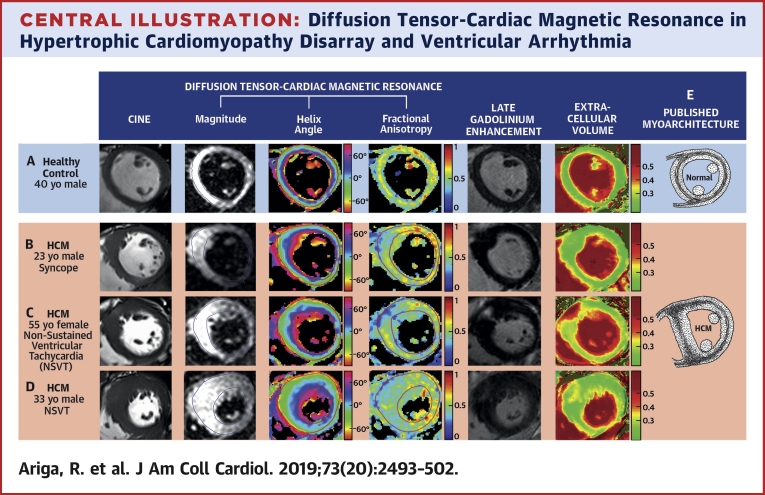
Background: Myocardial disarray is a likely focus for fatal arrhythmia in hypertrophic cardiomyopathy (HCM). This microstructural abnormality can be inferred by mapping the preferential diffusion of water along cardiac muscle fibers using diffusion tensor cardiac magnetic resonance (DT-CMR) imaging. Fractional anisotropy (FA) quantifies directionality of diffusion in 3 dimensions. The authors hypothesized that FA would be reduced in HCM due to disarray and fibrosis that may represent the anatomic substrate for ventricular arrhythmia.
Objectives: This study sought to assess FA as a noninvasive in vivo biomarker of HCM myoarchitecture and its association with ventricular arrhythmia.
Methods: A total of 50 HCM patients (47 ± 15 years of age, 77% male) and 30 healthy control subjects (46 ± 16 years of age, 70% male) underwent DT-CMR in diastole, cine, late gadolinium enhancement (LGE), and extracellular volume (ECV) imaging at 3-T.
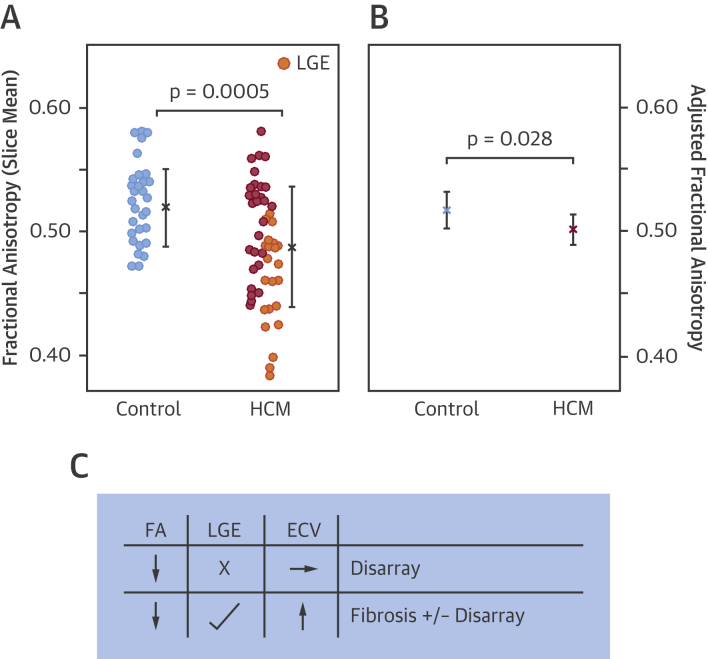
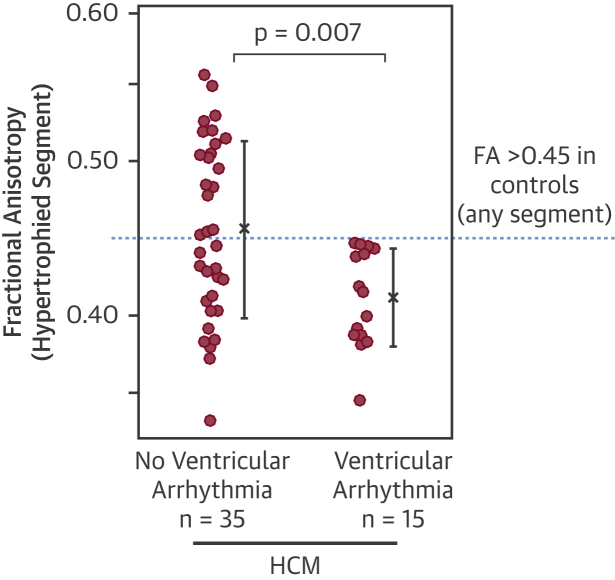
Results: Diastolic FA was reduced in HCM compared with control subjects (0.49 ± 0.05 vs. 0.52 ± 0.03; p = 0.0005). Control subjects had a mid-wall ring of high FA. In HCM, this ring was disrupted by reduced FA, consistent with published histology demonstrating that disarray and fibrosis invade circumferentially aligned mid-wall myocytes. LGE and ECV were significant predictors of FA, in line with fibrosis contributing to low FA. Yet FA adjusted for LGE and ECV remained reduced in HCM (p = 0.028). FA in the hypertrophied segment was reduced in HCM patients with ventricular arrhythmia compared to patients without (n = 15; 0.41 ± 0.03 vs. 0.46 ± 0.06; p = 0.007). A decrease in FA of 0.05 increased odds of ventricular arrhythmia by 2.5 (95% confidence interval: 1.2 to 5.3; p = 0.015) in HCM and remained significant even after correcting for LGE, ECV, and wall thickness (p = 0.036).
Conclusions: DT-CMR assessment of left ventricular myoarchitecture matched patterns reported previously on histology. Low diastolic FA in HCM was associated with ventricular arrhythmia and is likely to represent disarray after accounting for fibrosis. The authors propose that diastolic FA could be the first in vivo marker of disarray in HCM and a potential independent risk factor.
Keywords: diffusion tensor cardiac magnetic resonance imaging; disarray; fractional anisotropy; hypertrophic cardiomyopathy; risk stratification; sudden cardiac death; ventricular arrhythmia.
Copyright © 2019. Published by Elsevier Inc.
Figures
Comment in
-
Understanding the Myocardial Architecture of Hypertrophic Cardiomyopathy for Clinical Care.J Am Coll Cardiol. 2019 May 28;73(20):2503-2505. doi: 10.1016/j.jacc.2019.03.466. J Am Coll Cardiol. 2019. PMID: 31118143 No abstract available.
-
CMR Assessment of Myocyte Disarray in HCM: Matching Another Piece in the Puzzle.J Am Coll Cardiol. 2019 Oct 8;74(14):1847-1848. doi: 10.1016/j.jacc.2019.06.079. J Am Coll Cardiol. 2019. PMID: 31582148 No abstract available.
References
-
- Maron B.J., Olivotto I., Spirito P. Epidemiology of hypertrophic cardiomyopathy–related death. Circulation. 2000;102:858–864. - PubMed
-
- Maron B.J., Casey S.A., Chan R.H., Garberich R.F., Rowin E.J., Maron M.S. Independent assessment of the European Society of Cardiology sudden death risk model for hypertrophic cardiomyopathy. Am J Cardiol. 2015;116:757–764. - PubMed
-
- O'Mahony C., Tome-Esteban M., Lambiase P.D. A validation study of the 2003 American College of Cardiology/European Society of Cardiology and 2011 American College of Cardiology Foundation/American Heart Association risk stratification and treatment algorithms for sudden cardiac death in patients with hypertrophic cardiomyopathy. Heart. 2013;99:534–541. - PubMed
-
- Varnava A.M., Elliott P.M., Mahon N., Davies M.J., McKenna W.J. Relation between myocyte disarray and outcome in hypertrophic cardiomyopathy. Am J Cardiol. 2001;88:275–279. - PubMed
-
- Varnava A.M., Elliott P.M., Baboonian C., Davison F., Davies M.J., McKenna W.J. Hypertrophic cardiomyopathy: histopathological features of sudden death in cardiac troponin T disease. Circulation. 2001;104:1380–1384. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
