

Utilization of computerized clinical decision support for potentially inappropriate medications
- PMID: 31118596
- PMCID: PMC6500432
- DOI: 10.2147/CIA.S192927
Utilization of computerized clinical decision support for potentially inappropriate medications
Abstract
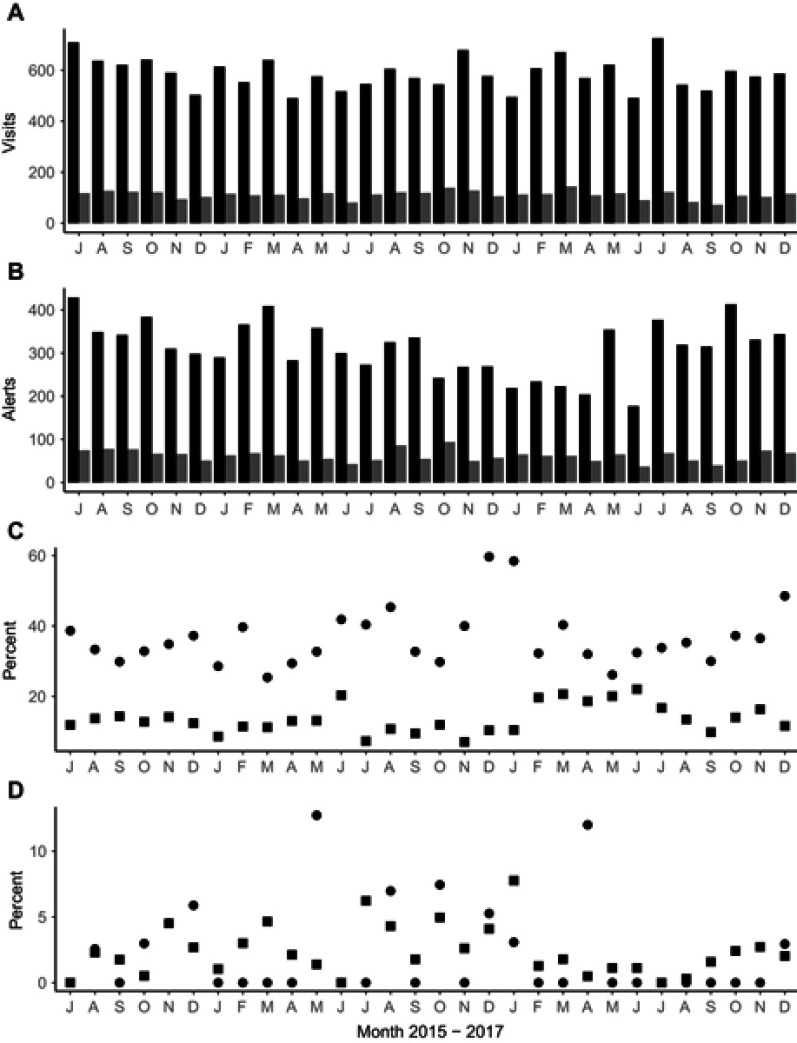
Background: Electronic medical record (EMR) alerts may inform point of care decisions, including the decision to prescribe potentially inappropriate medications (PIM) identified in the Beers criteria. EMR alerts may not be considered relevant or informative in the clinician context, leading to a phenomenon colloquially known as "alert fatigue." Objective: To assess the frequency of clinical interaction with EMR alerts and associated deprescribing behaviors in ambulatory settings. Methods: This is a retrospective observational study in two ambulatory clinics (the Kaye Edmonton Clinic Senior's Clinic and the Lynnwood Family Practice Clinic) in Edmonton over an observational period of 30 months. Statistical analysis was done using descriptive statistics, chi-square and regression analysis. Results: The reminder performance for interactions with the alert was 17.2% across the two clinics. The Number Needed to Remind (NNR) or mean number of alerts shown on clinician screens prior to a single interaction of any kind with the alert was 5.8. When actions were defined as a deprescribing (ie discontinuation) event that was related to the alert and that particular interaction in the EMR, the reminder performance was 1.2%, for an NNR of 82.8. Conclusion: The configuration of alerts in the EMR was not associated with a clinically detectable increase in the uptake of the Beers criteria for high hazard medications.
Keywords: Beers Criteria; alert fatigue; best practice advisory; deprescribing; e-prescribing; polypharmacy; prescribing.
Conflict of interest statement
Dr Allen Ausford reports consulting fees for clinical development work on the province of Alberta HIE(netcare)and CIS(eCLINICIAN- the ambulatory program that was used in this study) from Alberta Health Services, during the conduct of the study. Dr Jacques Romney received grants from University of Alberta eClinician EMR Innovation Grant, during the conduct of the study. The authors report no other conflicts of interest in this work.
Figures
References
-
- Scott IA, Anderson K, Freeman CR, Stowasser DA. First to do no harm. A real need to deprescribe in older patients. Med J Aust. 2014;201(7):390–392. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
