

The genomic architecture of antimalarial drug resistance
- PMID: 31119263
- PMCID: PMC6859814
- DOI: 10.1093/bfgp/elz008
The genomic architecture of antimalarial drug resistance
Abstract
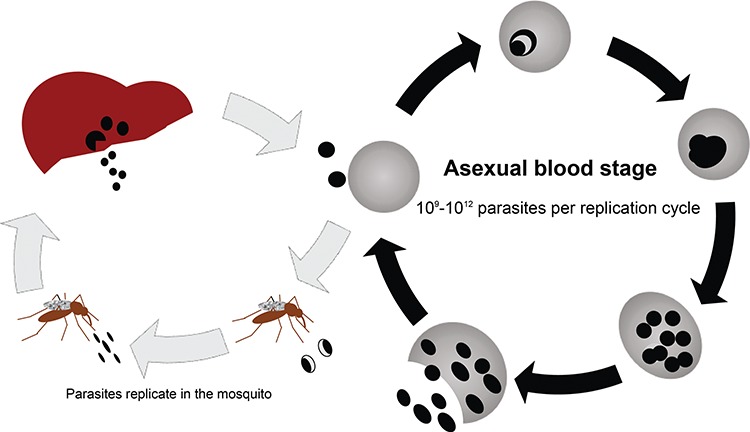
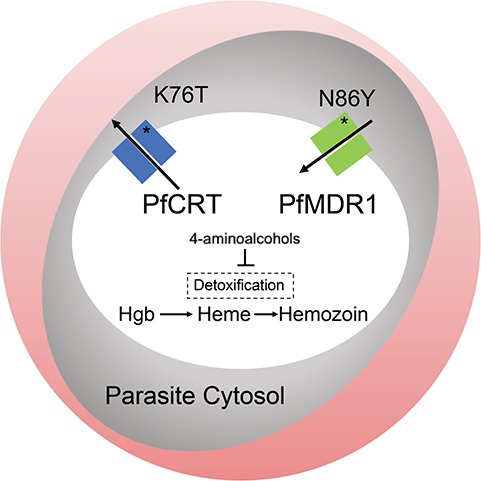
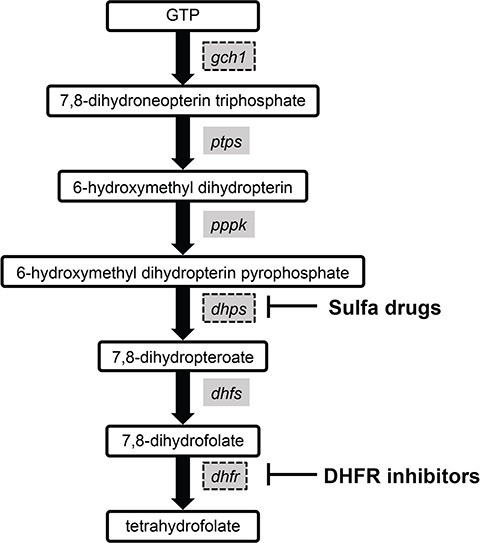
Plasmodium falciparum and Plasmodium vivax, the two protozoan parasite species that cause the majority of cases of human malaria, have developed resistance to nearly all known antimalarials. The ability of malaria parasites to develop resistance is primarily due to the high numbers of parasites in the infected person's bloodstream during the asexual blood stage of infection in conjunction with the mutability of their genomes. Identifying the genetic mutations that mediate antimalarial resistance has deepened our understanding of how the parasites evade our treatments and reveals molecular markers that can be used to track the emergence of resistance in clinical samples. In this review, we examine known genetic mutations that lead to resistance to the major classes of antimalarial medications: the 4-aminoquinolines (chloroquine, amodiaquine and piperaquine), antifolate drugs, aryl amino-alcohols (quinine, lumefantrine and mefloquine), artemisinin compounds, antibiotics (clindamycin and doxycycline) and a napthoquinone (atovaquone). We discuss how the evolution of antimalarial resistance informs strategies to design the next generation of antimalarial therapies.
Keywords: Plasmodium falciparum; Plasmodium vivax; artemisinin; drug resistance; malaria.
© The Author(s) 2019. Published by Oxford University Press.
Figures
References
-
- Korenromp EL, Williams BG, Gouws E, et al. Measurement of trends in childhood malaria mortality in Africa: an assessment of progress toward targets based on verbal autopsy. Lancet Infect Dis 2003;3:349–358. - PubMed
-
- World Health Organization Artemisinin and Artemisinin-Based Combination Therapy Resistance. Geneva, Switzerland, 2017.
-
- Maxmen A. How to defuse malaria’s ticking time bomb. Nature 2018;559:458–465. - PubMed
-
- World Health Organization Guidelines for the Treatment of Malaria, 3rd edn Geneva, Switzerland, 2015.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
