Effects of cannabinoid administration for pain: A meta-analysis and meta-regression
- PMID: 31120281
- PMCID: PMC6663642
- DOI: 10.1037/pha0000281
Effects of cannabinoid administration for pain: A meta-analysis and meta-regression
Abstract
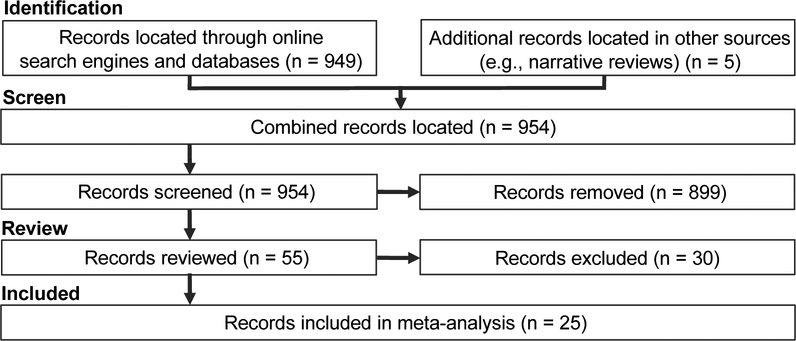
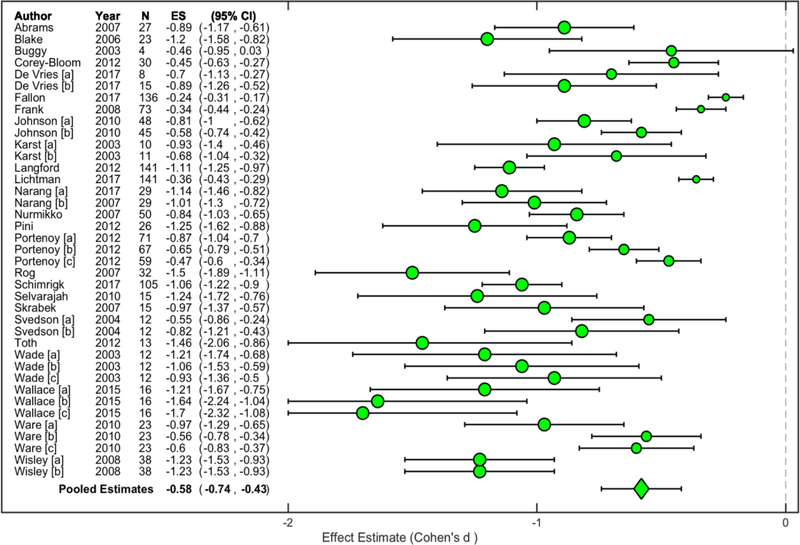
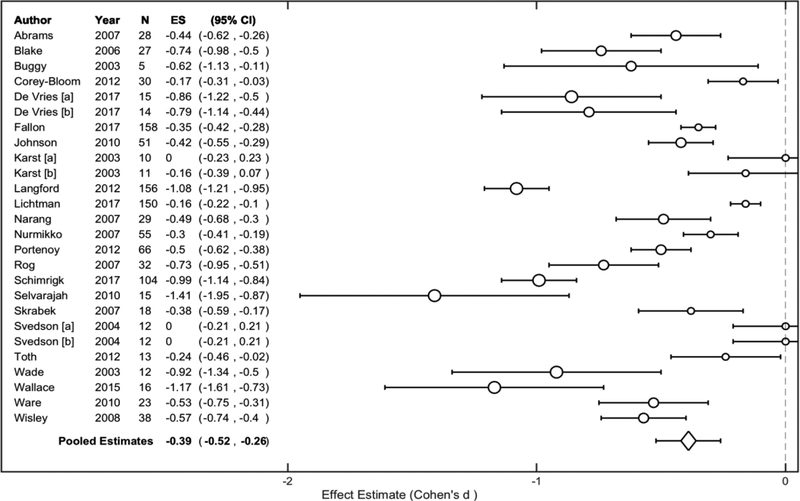
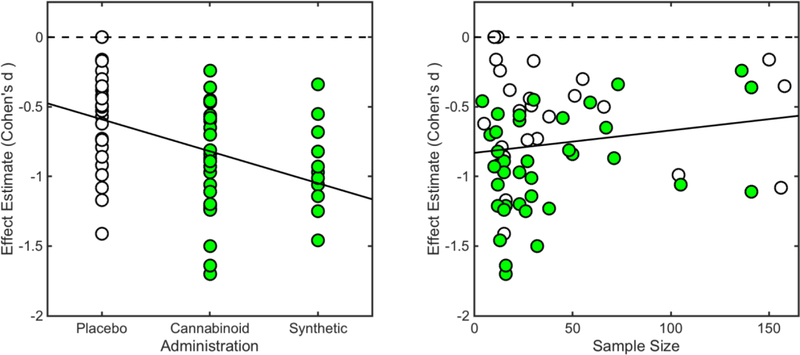
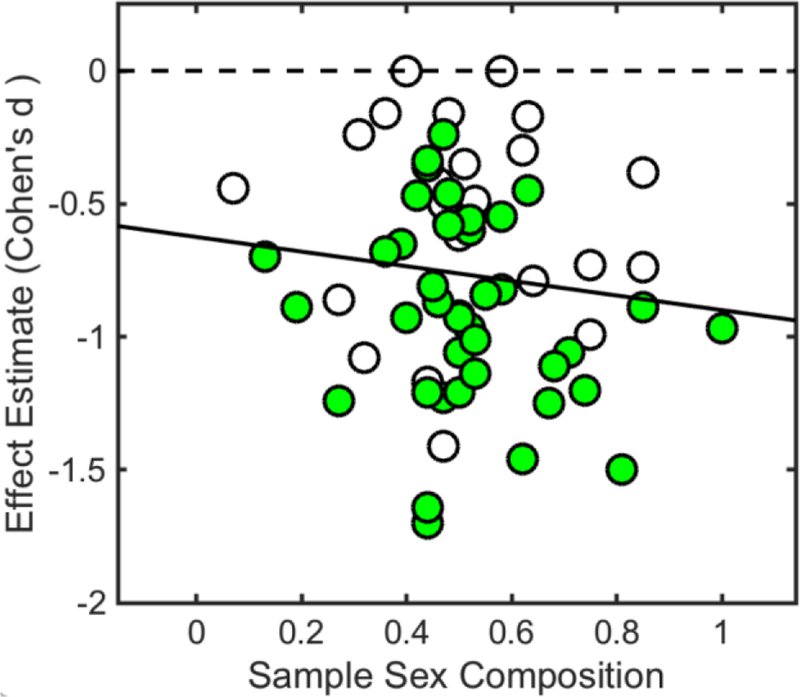
Chronic pain states have resulted in an overreliance on opioid pain relievers, which can carry significant risks when used long term. As such, alternative pain treatments are increasingly desired. Although emerging research suggests that cannabinoids have therapeutic potential regarding pain, results from studies across pain populations have been inconsistent. To provide meta-analytic clarification regarding cannabis's impact on subjective pain, we identified studies that assessed drug-induced pain modulations under cannabinoid and corresponding placebo conditions. A literature search yielded 25 peer-reviewed records that underwent data extraction. Baseline and end-point data were used to compute standardized effect size estimates (Cohen's d) across cannabinoid administrations (k = 39) and placebo administrations (k = 26). Standardized effects were inverse-variance weighted and pooled across studies for meta-analytic comparison. Results revealed that cannabinoid administration produced a medium-to-large effect across included studies, Cohen's d = -0.58, 95% confidence interval (CI) [-0.74, -0.43], while placebo administration produced a small-to-medium effect, Cohen's d = -0.39, 95% CI [-0.52, -0.26]. Meta-regression revealed that cannabinoids, β = -0.43, 95% CI [-0.62, -0.24], p < .05, synthetic cannabinoids, β = -0.39, 95% CI [-0.65, -0.14], p < .05, and sample size, β = 0.01, 95% CI [0.00, 0.01], p < .05, were associated with marked pain reduction. These outcomes suggest that cannabinoid-based pharmacotherapies may serve as effective replacement/adjunctive options regarding pain, however, additional research is warranted. Additionally, given demonstrated neurocognitive side effects associated with some constituent cannabinoids (i.e., THC), subsequent work may consider developing novel therapeutic agents that capitalize on cannabis's analgesic properties without producing adverse effects. (PsycINFO Database Record (c) 2019 APA, all rights reserved).
Figures
Similar articles
-
Opioid-sparing effect of cannabinoids for analgesia: an updated systematic review and meta-analysis of preclinical and clinical studies.Neuropsychopharmacology. 2022 Jun;47(7):1315-1330. doi: 10.1038/s41386-022-01322-4. Epub 2022 Apr 22. Neuropsychopharmacology. 2022. PMID: 35459926 Free PMC article.
-
Association of Cannabinoid Administration With Experimental Pain in Healthy Adults: A Systematic Review and Meta-analysis.JAMA Psychiatry. 2018 Nov 1;75(11):1118-1127. doi: 10.1001/jamapsychiatry.2018.2503. JAMA Psychiatry. 2018. PMID: 30422266 Free PMC article.
-
Cannabis and cannabinoids for the treatment of people with chronic noncancer pain conditions: a systematic review and meta-analysis of controlled and observational studies.Pain. 2018 Oct;159(10):1932-1954. doi: 10.1097/j.pain.0000000000001293. Pain. 2018. PMID: 29847469
-
Synergistic interactions between cannabinoid and opioid analgesics.Life Sci. 2004 Jan 30;74(11):1317-24. doi: 10.1016/j.lfs.2003.09.038. Life Sci. 2004. PMID: 14706563 Review.
-
Therapeutic potential of cannabinoids in CNS disease.CNS Drugs. 2003;17(3):179-202. doi: 10.2165/00023210-200317030-00004. CNS Drugs. 2003. PMID: 12617697 Review.
Cited by
-
Chronic Pain and Cannabis Use Frequency, Intensity, and Severity in Young Adults.Subst Use Misuse. 2024;59(4):576-582. doi: 10.1080/10826084.2023.2287240. Epub 2024 Feb 8. Subst Use Misuse. 2024. PMID: 38017655 Free PMC article.
-
Cannabinoids: Potential for Modulation and Enhancement When Combined with Vitamin B12 in Case of Neurodegenerative Disorders.Pharmaceuticals (Basel). 2024 Jun 20;17(6):813. doi: 10.3390/ph17060813. Pharmaceuticals (Basel). 2024. PMID: 38931480 Free PMC article. Review.
-
The role of prescription opioid and cannabis supply policies on opioid overdose deaths.Am J Epidemiol. 2025 Mar 4;194(3):791-801. doi: 10.1093/aje/kwae210. Am J Epidemiol. 2025. PMID: 39030721 Free PMC article.
-
Opioid Use in Patients With Cervical Cancer at Two Urban Medical Centers.Adv Radiat Oncol. 2021 Oct 20;7(2):100833. doi: 10.1016/j.adro.2021.100833. eCollection 2022 Mar-Apr. Adv Radiat Oncol. 2021. PMID: 35387422 Free PMC article.
-
Cannabinoids in the descending pain modulatory circuit: Role in inflammation.Pharmacol Ther. 2020 May;209:107495. doi: 10.1016/j.pharmthera.2020.107495. Epub 2020 Jan 29. Pharmacol Ther. 2020. PMID: 32004514 Free PMC article. Review.
References
-
- Abrams DI, Jay CA, Shade SB, Vizoso H, Reda H, Press S, … Petersen KL (2007). Cannabis in Painful HIV-associated Neuropathy: a randomized placebo-controlled clinical trial. Neurology, 68(7), 515–521. - PubMed
-
- Aviram J, & Samuelly-Leichtag G (2017). Efficacy of Cannabis-Based Medicines for Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pain Physician, 20(6), E755–E796. - PubMed
-
- Baker WL, White CM, Cappelleri JC, Kluger J, Coleman CI, Health Outcomes, P., & Economics Collaborative, G. (2009). Understanding heterogeneity in meta-analysis: the role of meta-regression. International Journal of Clinical Practice, 63(10), 1426–1434. doi:10.1111/j.1742-1241.2009.02168.x - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials