

Effect of Gemcitabine and nab-Paclitaxel With or Without Hydroxychloroquine on Patients With Advanced Pancreatic Cancer: A Phase 2 Randomized Clinical Trial
- PMID: 31120501
- PMCID: PMC6547080
- DOI: 10.1001/jamaoncol.2019.0684
Effect of Gemcitabine and nab-Paclitaxel With or Without Hydroxychloroquine on Patients With Advanced Pancreatic Cancer: A Phase 2 Randomized Clinical Trial
Abstract
Importance: Autophagy is a mechanism of treatment resistance to chemotherapy that has a role in the maintenance of pancreatic cancer. Hydroxychloroquine sulfate (HCQ) is an inhibitor of autophagy that inhibits the fusion of the autophagosome to the lysosome.
Objective: To determine whether HCQ improves overall survival at 1 year in combination with gemcitabine hydrochloride and nab-paclitaxel (GA) among patients with metastatic pancreatic cancer.
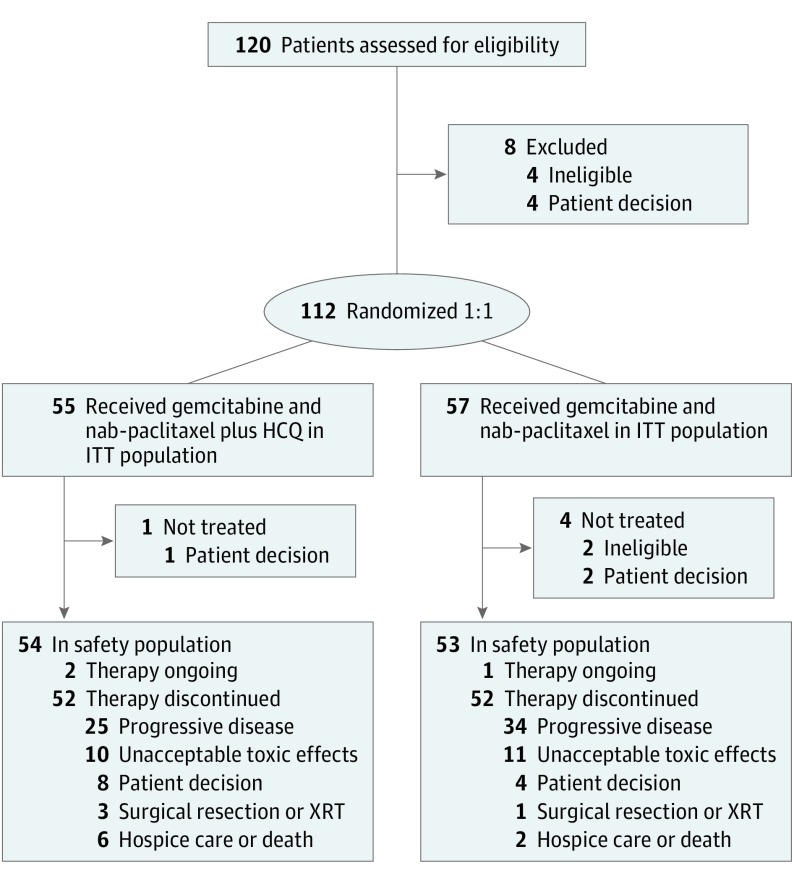
Design, setting, and participants: Open-label, phase 2 randomized clinical trial conducted between March 18, 2013, and November 16, 2017, at the University of Pennsylvania, HonorHealth, and The Johns Hopkins University among 112 patients with previously untreated metastatic or advanced pancreatic ductal adenocarcinoma, Eastern Cooperative Oncology Group performance status of 0 or 1, and adequate marrow and organ function. All efficacy analyses were performed for the intention-to-treat population.
Interventions: Patients were randomized in a 1:1 ratio to receive GA with or without HCQ. All patients received standard doses of GA, and those randomized to receive HCQ were treated continuously with 600 mg orally twice daily.
Main outcome and measure: Overall survival at 1 year.
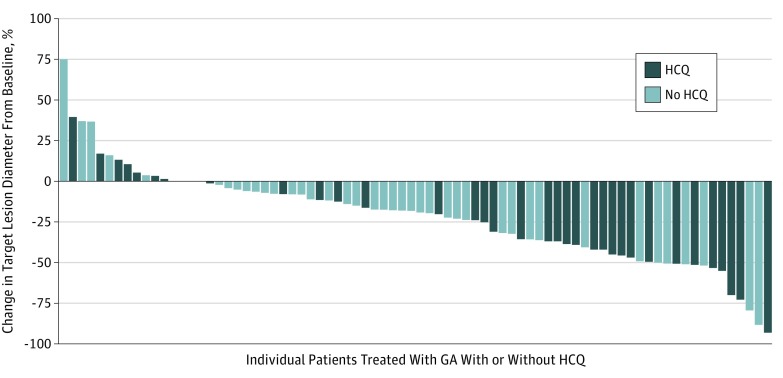
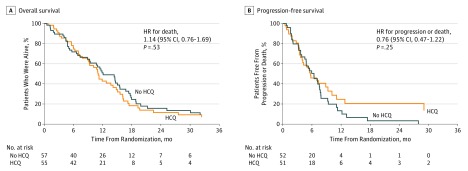
Results: A total of 112 patients (45 women and 67 men; median age, 65 years; range, 43-86 years) were enrolled; 55 were randomized to receive GA plus HCQ, and 57 to receive GA. Overall survival at 12 months was 41% (95% CI, 27%-53%) in the HCQ group and 49% (95% CI, 35%-61%) in the non-HCQ group. Median progression-free survival was 5.7 months (95% CI, 4.0-9.3 months) in the HCQ group and 6.4 months (95% CI, 4.5-7.6 months) in the non-HCQ group. Median overall survival was 11.1 months (95% CI, 9.0-14.2 months) in the HCQ group and 12.1 months (95% CI, 9.3-15.5 months) in the non-HCQ group. Overall response rate was 38.2% (n = 21) in the HCQ group and 21.1% (n = 12) in the non-HCQ group (P = .047). Treatment-related grade 3 or 4 adverse events that differed between the HCQ and non-HCQ groups were neutropenia (23 of 54 [42.6%] vs 12 of 53 [22.6%]), anemia (2 of 54 [3.7%] vs 9 of 53 [17.0%]), fatigue (4 of 54 [7.4%] vs 0), nausea (5 of 54 [9.3%] vs 0), peripheral neuropathy (7 of 54 [13.0%] vs 3 of 53 [5.7%]), visual changes (3 of 54 [5.6%] vs 0), and neuropsychiatric symptoms (3 of 54 [5.6%] vs 0).
Conclusions and relevance: The addition of HCQ to block autophagy did not improve the primary end point of overall survival at 12 months. These data do not support the routine use of GA plus HCQ for metastatic pancreatic cancer in the absence of a biomarker. However, improvement seen in the overall response rate with HCQ may indicate a role for HCQ in the locally advanced setting, where tumor response may permit resection.
Trial registration: ClinicalTrials.gov identifier: NCT01506973.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
