Metabolic, mitochondrial, renal and hepatic safety of enfuvirtide and raltegravir antiretroviral administration: Randomized crossover clinical trial in healthy volunteers
- PMID: 31120908
- PMCID: PMC6532851
- DOI: 10.1371/journal.pone.0216712
Metabolic, mitochondrial, renal and hepatic safety of enfuvirtide and raltegravir antiretroviral administration: Randomized crossover clinical trial in healthy volunteers
Abstract
Context: Classical antiretroviral agents may acutely impact on metabolic, mitochondrial, renal and hepatic function in HIV-infected and uninfected persons. Fusion and integrase inhibitors are supposed to be safer, but have been scarcely investigated. To avoid any interference with HIV or other antiretrovirals, we assessed markers of these toxicities in healthy adult volunteers treated with Enfuvirtide (T20) or Raltegravir (RAL).
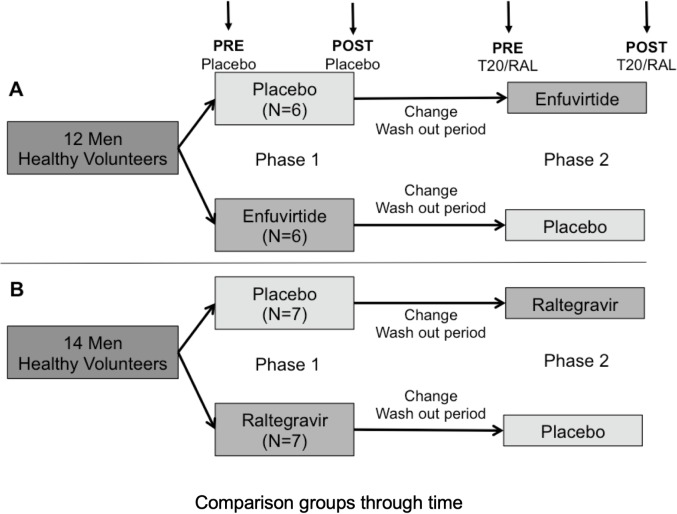
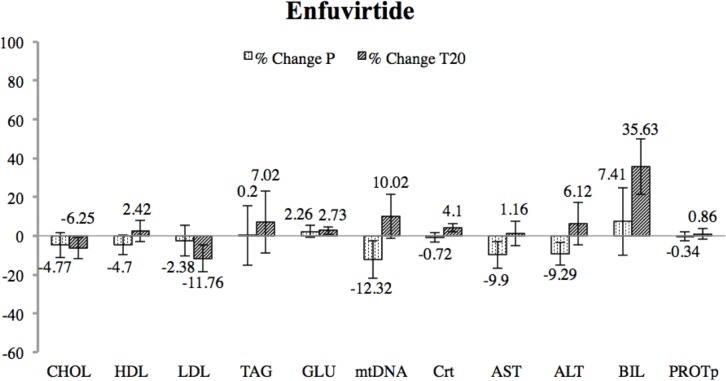
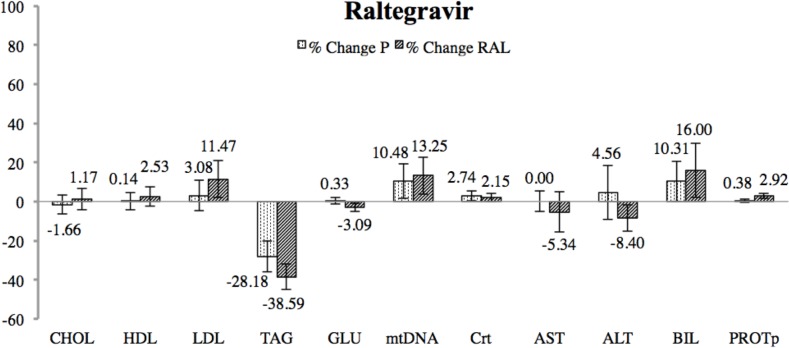
Methods: Twenty-six healthy participants were randomized to T20/90mg vs. placebo (n = 12) or RAL/400mg vs. placebo (n = 14) every 12h in two 7-day periods separated by a 4-week washout period. Major end-points were changes in lipid profile (total cholesterol, high-density-lipoprotein (HDL)-cholesterol, low-density-lipoprotein (LDL)-cholesterol, triglycerides), insulin resistance (glucose) and mitochondrial toxicity (mitochondrial DNA content-mtDNA-in peripheral blood mononuclear cells). Renal and hepatic toxicity (creatinine, alanine transaminase (AST), alanine aminotransferase (ALT), bilirubin and total plasma proteins) and overall safety were also analysed. Effect of period, treatment, and basal measures were evaluated for each end-point.
Results: Neither T20-administration nor RAL-administration yielded to any statistic significant change in the markers of metabolic, mitochondrial, renal or hepatic toxicity assessed. No symptoms indicative of drug toxicity were neither found in any subject.
Conclusions: In absence of HIV infection, or concomitant treatment, short-term exposure to T20 or RAL in healthy adult volunteers did not lead to any indicative changes in toxicity markers thus presuming the safe profile of both drugs.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures