

Is prehospital endobronchial intubation a risk factor for subsequent ventilator associated pneumonia? A retrospective analysis
- PMID: 31120987
- PMCID: PMC6532927
- DOI: 10.1371/journal.pone.0217466
Is prehospital endobronchial intubation a risk factor for subsequent ventilator associated pneumonia? A retrospective analysis
Abstract
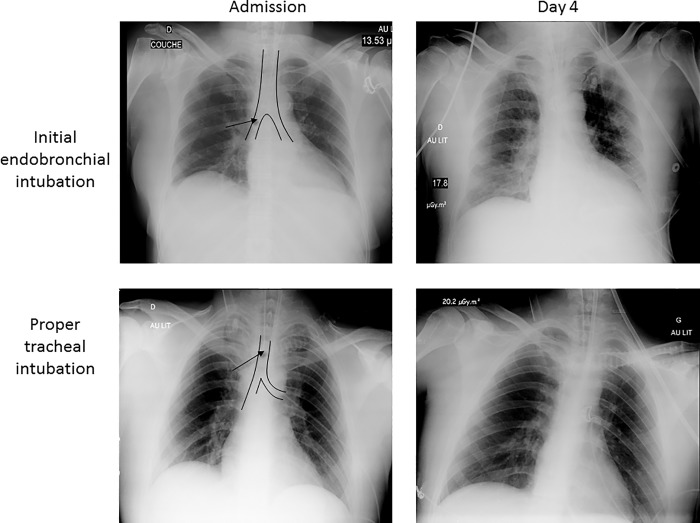
More than half of patients under mechanical ventilation in the intensive care unit (ICU) are field-intubated, which is a known risk factor for ventilator associated pneumonia (VAP). We assessed whether field endobronchial intubation (EBI) is associated with the development of subsequent VAP during the ICU stay. This retrospective, nested case-control study was conducted in a cohort of field-intubated patients admitted to an ICU of a teaching hospital during a three-year period. Cases were defined as field-intubated patients with EBI and controls corresponded to field-intubated patients with proper position of the tracheal tube on admission chest X-ray. Primary endpoint was the development of early VAP. Secondary endpoints included the development of early ventilator associated tracheo-bronchitis, late VAP, duration of mechanical ventilation, length of stay and mortality in the ICU. A total of 145 patients were studied (mean age: 54 ± 19 years; men: 74%). Reasons for field intubation were predominantly multiple trauma (49%) and cardiorespiratory arrest (38%). EBI was identified in 33 patients (23%). Fifty-three patients (37%) developed early or late VAP. EBI after field intubation was associated with a nearly two-fold increase of early VAP, though not statistically significant (30% vs. 17%: p = 0.09). No statistically significant difference was found regarding secondary outcomes. The present study suggests that inadvertent prehospital EBI could be associated with a higher incidence of early-onset VAP. Larger studies are required to confirm this hypothesis. Whether strategies aimed at decreasing the incidence and duration of EBI could reduce the incidence of subsequent VAP remains to be determined.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Safdar N, Dezfulian C, Collard HR, Saint S. Clinical and economic consequences of ventilator-associated pneumonia: a systematic review. Crit Care Med. 2005;33: 2184–2193. - PubMed
-
- Kalil AC, Metersky ML, Klompas M, Muscedere J, Sweeney DA, Palmer LB, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63: e61–e111. 10.1093/cid/ciw353 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
