

Spread Through Air Spaces (STAS) Is Prognostic in Atypical Carcinoid, Large Cell Neuroendocrine Carcinoma, and Small Cell Carcinoma of the Lung
- PMID: 31121325
- PMCID: PMC8160527
- DOI: 10.1016/j.jtho.2019.05.009
Spread Through Air Spaces (STAS) Is Prognostic in Atypical Carcinoid, Large Cell Neuroendocrine Carcinoma, and Small Cell Carcinoma of the Lung
Abstract
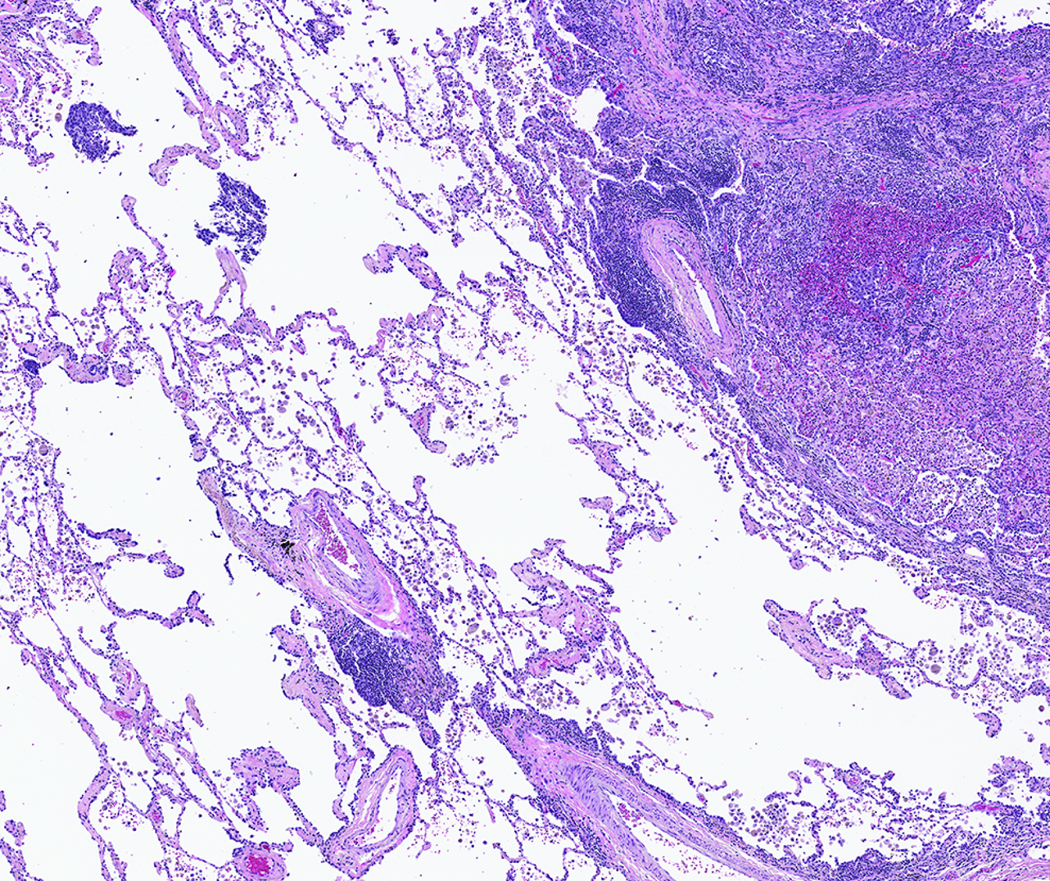
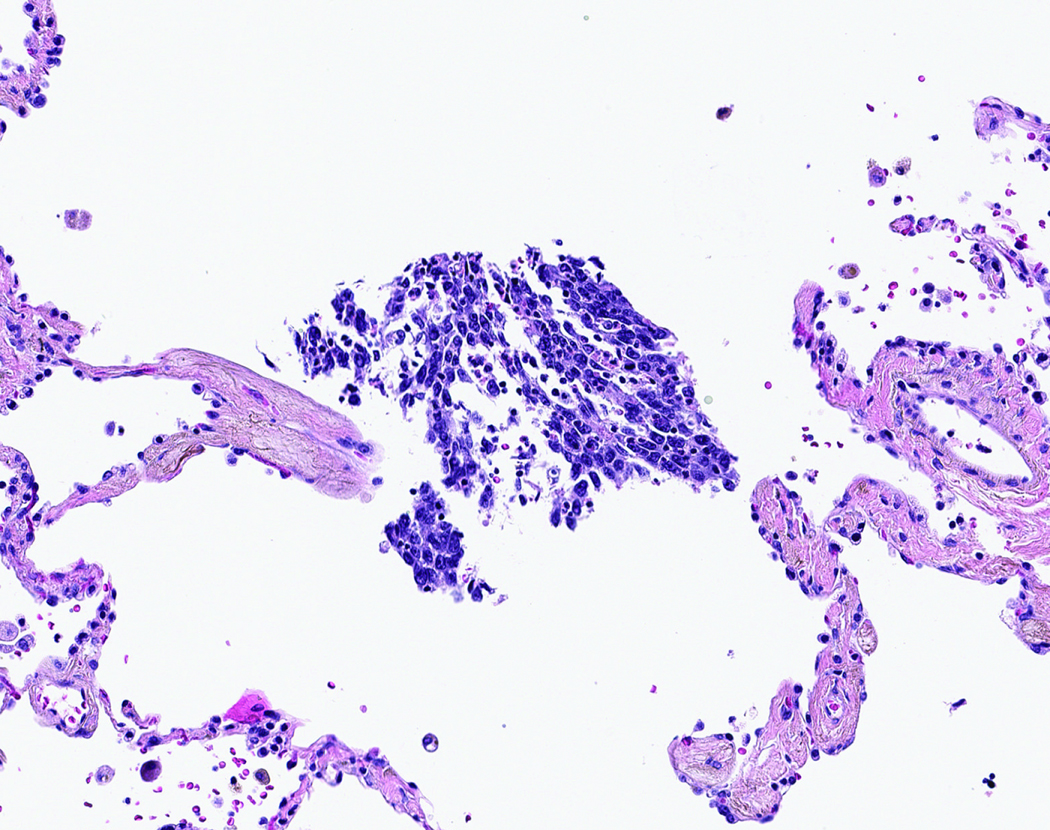
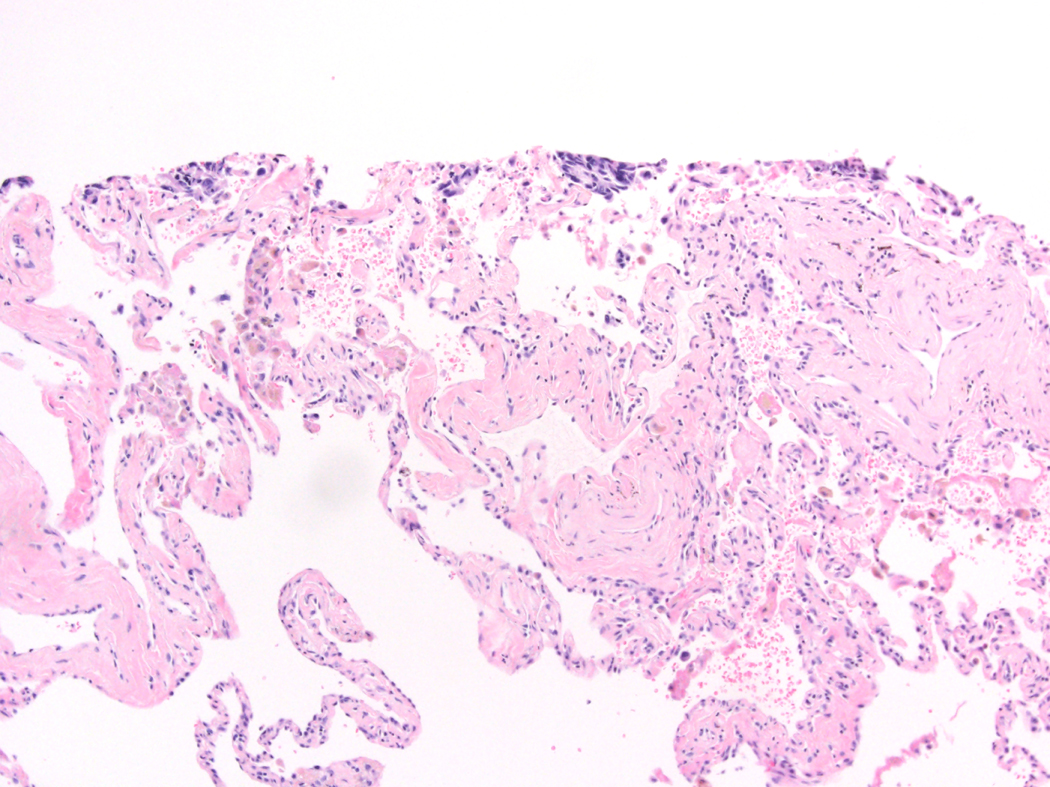
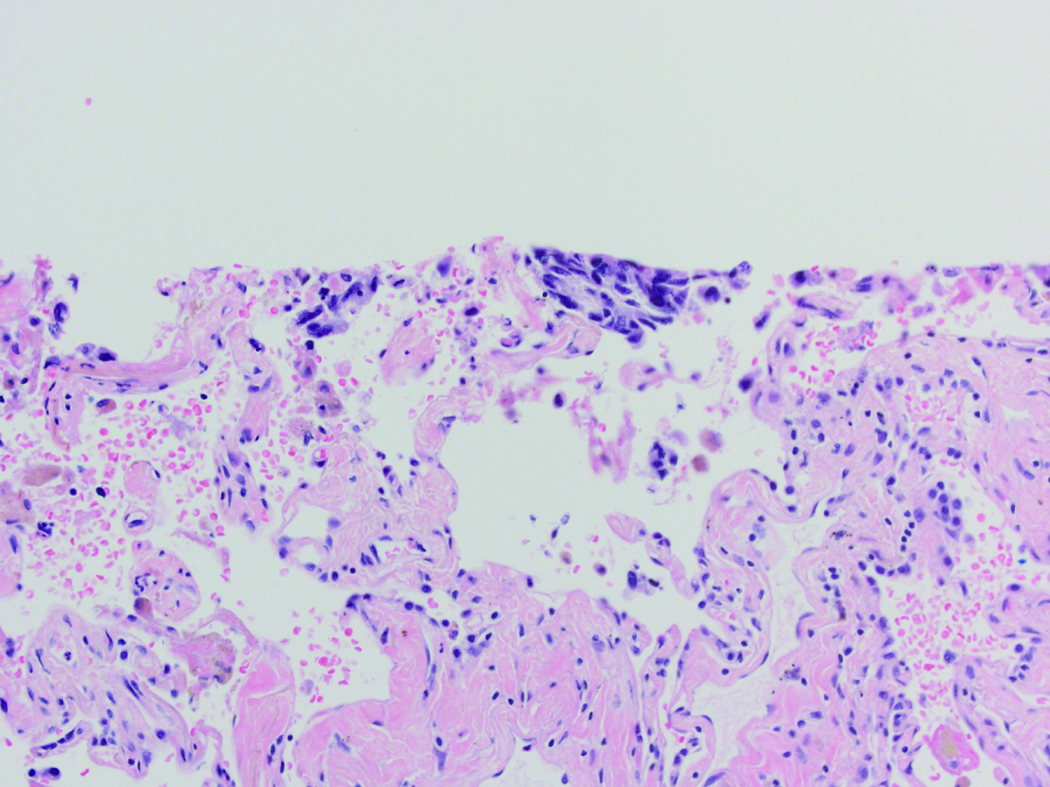
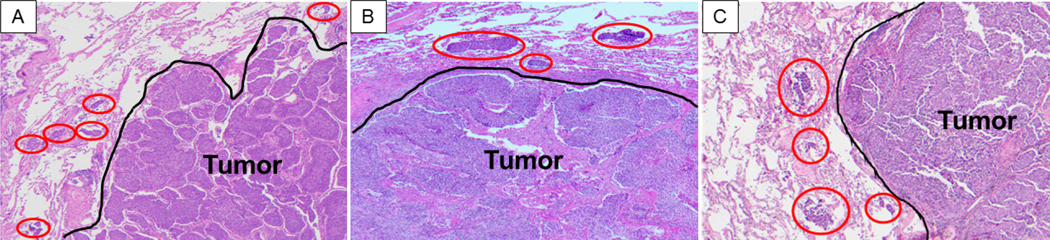
Introduction: Tumor spread through air spaces (STAS) has prognostic significance in lung adenocarcinoma and squamous cell carcinoma. We sought to investigate the prognostic importance of STAS in lung neuroendocrine tumors (NETs).
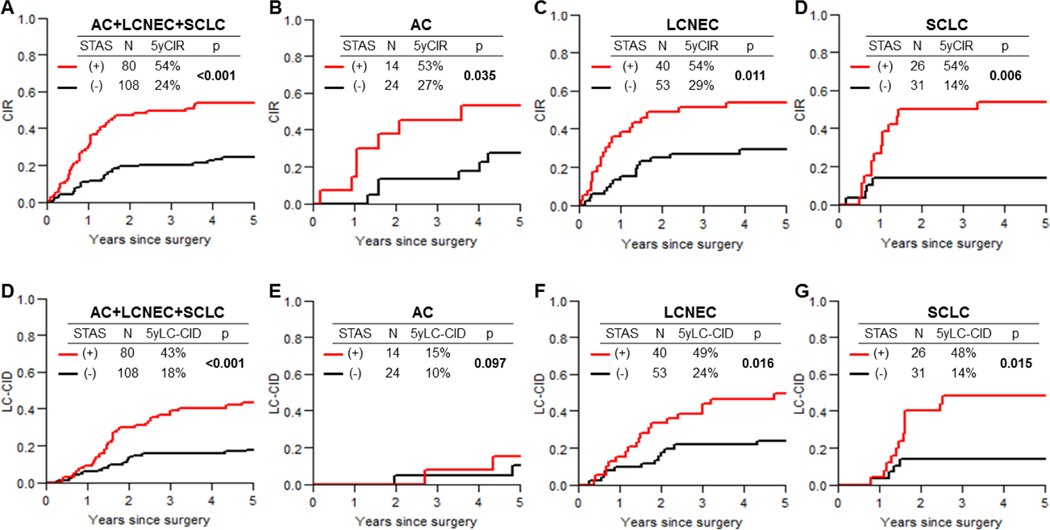
Methods: All tumor slides from patients with resected pathologic stage I to III lung NETs (N = 487) (299 with typical carcinoid [TC], 38 with atypical carcinoid [AC], 93 with large cell neuroendocrine carcinoma [LCNEC], and 57 with SCLC) treated between 1992 and 2012 were evaluated for presence of STAS. Cumulative incidence of recurrence (CIR) and lung cancer-specific cumulative incidence of death (LC-CID) were analyzed by using a competing-risks approach.
Results: STAS was identified in 26% of NETs (16% of TCs, 37% of ACs, 43% of LCNECs, and 46% of SCLCs). STAS was associated with distant metastasis, as well as with higher CIR and LC-CID in the overall cohort and in the AC, LCNEC, and SCLC cohorts (owing to a small number of recurrences and deaths [<5], prognostic analysis was not performed in the TC cohort). In multivariable analysis stratified by stage, STAS was significantly associated with higher CIR (subhazard ratio = 2.85, 95% confidence interval: 1.73-4.68, p < 0.001) and LC-CID (subhazard ratio = 2.72, 95% confidence interval: 1.57-4.70, p < 0.001), independent of histologic subtype. STAS was independently associated with CIR and LC-CID in the LCNEC cohort and LC-CID in the SCLC cohort.
Conclusions: In patients with lung NETs, STAS is associated with early distant metastasis and worse LC-CID. In patients with LCNEC or SCLC, STAS is an independent poor prognostic factor.
Keywords: Competing-risks analysis; Lung cancer–specific death; Lung neuroendocrine tumor; Recurrence; Spread through air spaces.
Copyright © 2019 International Association for the Study of Lung Cancer. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Spread through air spaces in lung neuroendocrine tumor.Transl Lung Cancer Res. 2019 Dec;8(Suppl 4):S439-S442. doi: 10.21037/tlcr.2019.10.20. Transl Lung Cancer Res. 2019. PMID: 32038933 Free PMC article. No abstract available.
-
Lung neuroendocrine tumors: a new addition to the evolving list of spread through air spaces.Transl Lung Cancer Res. 2019 Dec;8(Suppl 4):S443-S446. doi: 10.21037/tlcr.2019.09.03. Transl Lung Cancer Res. 2019. PMID: 32038934 Free PMC article. No abstract available.
-
RE: Spread Through Air Spaces (STAS) is Prognostic in Atypical Carcinoid, Large Cell Neuroendocrine Carcinoma, and Small Cell Carcinoma of the Lung.J Thorac Oncol. 2020 Jul;15(7):e116-e117. doi: 10.1016/j.jtho.2019.11.027. J Thorac Oncol. 2020. PMID: 32593449 No abstract available.
-
Spread Through Air Spaces Is Prognostic in Neuroendocrine Lung Tumors and Can Be Distinguished From Artifacts.J Thorac Oncol. 2020 Jul;15(7):e118-e120. doi: 10.1016/j.jtho.2020.04.017. J Thorac Oncol. 2020. PMID: 32593450 No abstract available.
Similar articles
-
Large cell neuroendocrine carcinoma of the lung: a histologic and immunohistochemical study of 22 cases.Am J Surg Pathol. 1998 May;22(5):526-37. doi: 10.1097/00000478-199805000-00002. Am J Surg Pathol. 1998. PMID: 9591721
-
Spread through air spaces (STAS) is a predictor of poor outcome in atypical carcinoids of the lung.Virchows Arch. 2019 Sep;475(3):325-334. doi: 10.1007/s00428-019-02596-8. Epub 2019 Jun 15. Virchows Arch. 2019. PMID: 31201506
-
Analysis of p53, K-ras-2, and C-raf-1 in pulmonary neuroendocrine tumors. Correlation with histological subtype and clinical outcome.Am J Pathol. 1996 May;148(5):1531-41. Am J Pathol. 1996. PMID: 8623922 Free PMC article.
-
Typical and atypical carcinoid tumors of the lung are characterized by 11q deletions as detected by comparative genomic hybridization.Am J Pathol. 1998 Oct;153(4):1089-98. doi: 10.1016/S0002-9440(10)65653-2. Am J Pathol. 1998. PMID: 9777940 Free PMC article. Review.
-
Molecular and cellular biology of neuroendocrine lung tumors: evidence for separate biological entities.Biochim Biophys Acta. 2012 Dec;1826(2):255-71. doi: 10.1016/j.bbcan.2012.05.001. Epub 2012 May 10. Biochim Biophys Acta. 2012. PMID: 22579738 Review.
Cited by
-
Prognostic Impact and Clinical Features of Spread through Air Spaces in Operated Lung Cancer: Real-World Analysis.Medicina (Kaunas). 2024 Aug 22;60(8):1374. doi: 10.3390/medicina60081374. Medicina (Kaunas). 2024. PMID: 39202654 Free PMC article.
-
Radiomics is feasible for prediction of spread through air spaces in patients with nonsmall cell lung cancer.Sci Rep. 2021 Jun 29;11(1):13526. doi: 10.1038/s41598-021-93002-4. Sci Rep. 2021. PMID: 34188146 Free PMC article.
-
Relevance and prognostic ability of Twist, Slug and tumor spread through air spaces in lung adenocarcinoma.Cancer Med. 2020 Mar;9(6):1986-1998. doi: 10.1002/cam4.2858. Epub 2020 Jan 22. Cancer Med. 2020. PMID: 31970942 Free PMC article.
-
Preoperative CT radiomic model combined with clinical and CT imaging features to predict the spread through air spaces in T1 invasive lung adenocarcinoma.Am J Transl Res. 2024 Oct 15;16(10):6106-6118. doi: 10.62347/UJYU8551. eCollection 2024. Am J Transl Res. 2024. PMID: 39544799 Free PMC article.
-
Tumor Spread Through Air Spaces Predicts Survival in Resected Pulmonary Lymphoepithelial Carcinoma.Ann Surg Oncol. 2025 Apr;32(4):2675-2686. doi: 10.1245/s10434-024-16401-7. Epub 2024 Nov 4. Ann Surg Oncol. 2025. PMID: 39495361
References
-
- Yao JC, Hassan M, Phan A, et al. One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. JClinOncol 2008;26:3063–72. - PubMed
-
- Travis WD. Advances in neuroendocrine lung tumors. AnnOncol 2010;21 Suppl 7:vii65-vii71. - PubMed
-
- Skuladottir H, Hirsch FR, Hansen HH, Olsen JH. Pulmonary neuroendocrine tumors: incidence and prognosis of histological subtypes. A population-based study in Denmark. Lung Cancer 2002;37:127–35. - PubMed
-
- Gustafsson BI, Kidd M, Chan A, Malfertheiner MV, Modlin IM. Bronchopulmonary neuroendocrine tumors. Cancer 2008;113:5–21. - PubMed
-
- Travis WD, Brambilla E, Burke AP, Marx A, Nicholson AG. WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart. 4th ed. Lyon: International Agency for Research on Cancer; 2015. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
