

Transthoracic Impedance Measured with Defibrillator Pads-New Interpretations of Signal Change Induced by Ventilations
- PMID: 31121817
- PMCID: PMC6571933
- DOI: 10.3390/jcm8050724
Transthoracic Impedance Measured with Defibrillator Pads-New Interpretations of Signal Change Induced by Ventilations
Abstract
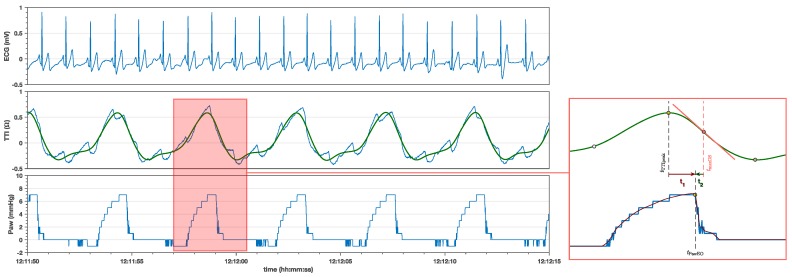
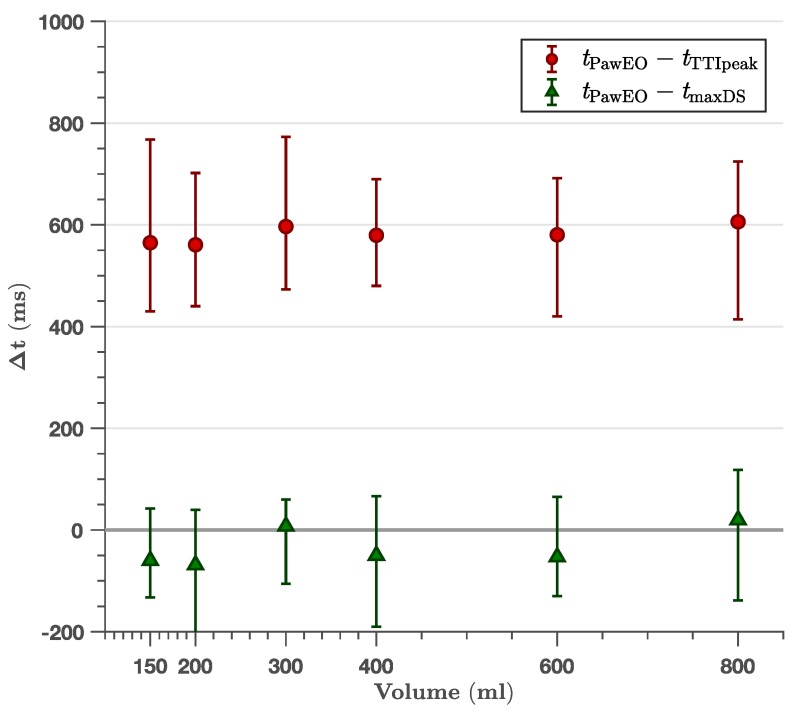
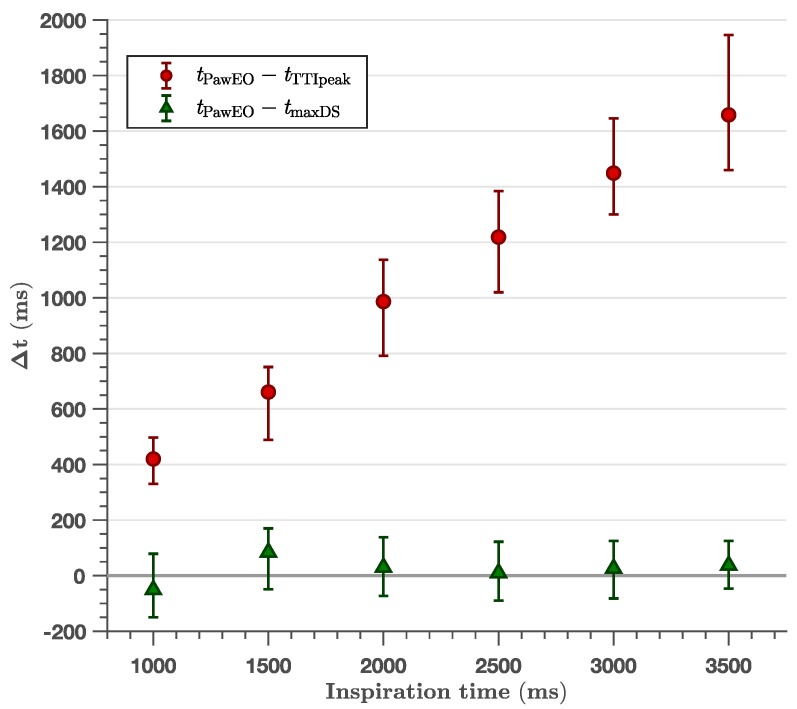
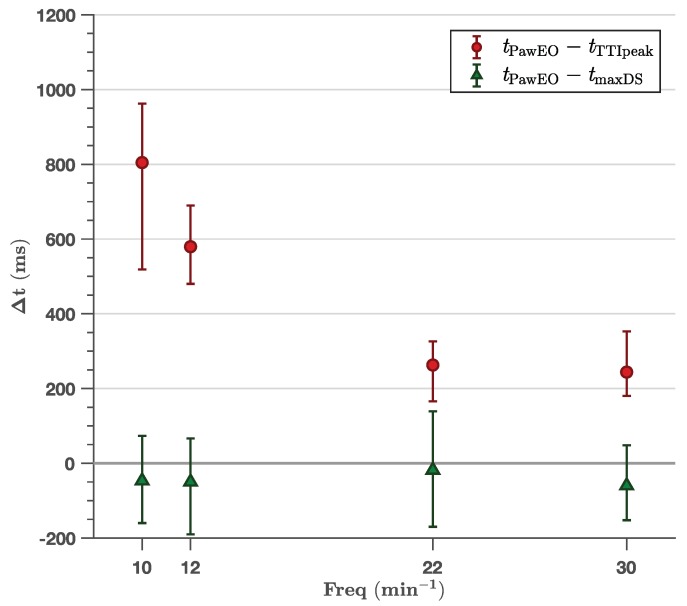
Compressions during the insufflation phase of ventilations may cause severe pulmonary injury during cardiopulmonary resuscitation (CPR). Transthoracic impedance (TTI) could be used to evaluate how chest compressions are aligned with ventilations if the insufflation phase could be identified in the TTI waveform without chest compression artifacts. Therefore, the aim of this study was to determine whether and how the insufflation phase could be precisely identified during TTI. We synchronously measured TTI and airway pressure (Paw) in 21 consenting anaesthetised patients, TTI through the defibrillator pads and Paw by connecting the monitor-defibrillator's pressure-line to the endotracheal tube filter. Volume control mode with seventeen different settings were used (5-10 ventilations/setting): Six volumes (150-800 mL) with 12 min-1 frequency, four frequencies (10, 12, 22 and 30 min-1) with 400 mL volume, and seven inspiratory times (0.5-3.5 s ) with 400 mL/10 min-1 volume/frequency. Median time differences (quartile range) between timing of expiration onset in the Paw-line (PawEO) and the TTI peak and TTI maximum downslope were measured. TTI peak and PawEO time difference was 579 (432-723) m s for 12 min-1, independent of volume, with a negative relation to frequency, and it increased linearly with inspiratory time (slope 0.47, R 2 = 0.72). PawEO and TTI maximum downslope time difference was between -69 and 84 m s for any ventilation setting (time aligned). It was independent ( R 2 < 0.01) of volume, frequency and inspiratory time, with global median values of -47 (-153-65) m s , -40 (-168-68) m s and 20 (-93-128) m s , for varying volume, frequency and inspiratory time, respectively. The TTI peak is not aligned with the start of exhalation, but the TTI maximum downslope is. This knowledge could help with identifying the ideal ventilation pattern during CPR.
Keywords: cardiopulmonary resuscitation (CPR); peak inspiration pressure; pulmonary barotrauma; pulmonary injury; transthoracic impedance; ventilation; ventilation pattern.
Conflict of interest statement
L.W. is the NAKOS representative in the Medical Advisory Board of Stryker and holds patents licensed to Stryker and Zoll. The other authors declare that they have no conflicts of interest related to the research.
Figures
References
-
- Monsieurs K.G., Nolan J.P., Bossaert L.L., Greif R., Maconochie I.K., Nikolaou N.I., Perkins G.D., Soar J., Truhlář A., Wyllie J., et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 1. Executive summary. Resuscitation. 2015;95:1–80. doi: 10.1016/j.resuscitation.2015.07.038. - DOI - PubMed
-
- Karagiannidis C., Waldmann A.D., Róka P.L., Schreiber T., Strassmann S., Windisch W., Böhm S.H. Regional expiratory time constants in severe respiratory failure estimated by electrical impedance tomography: A feasibility study. Crit. Care. 2018;22:221. doi: 10.1186/s13054-018-2137-3. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
