

Advance in the Management of Sepsis-Induced Coagulopathy and Disseminated Intravascular Coagulation
- PMID: 31121897
- PMCID: PMC6572234
- DOI: 10.3390/jcm8050728
Advance in the Management of Sepsis-Induced Coagulopathy and Disseminated Intravascular Coagulation
Abstract
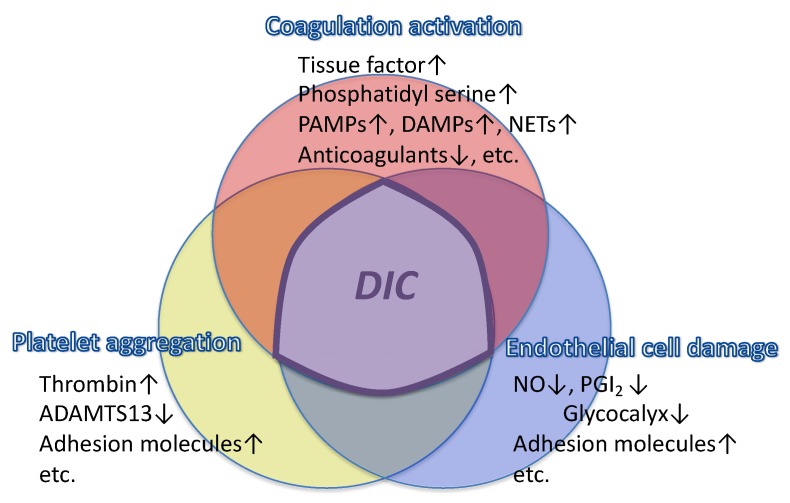
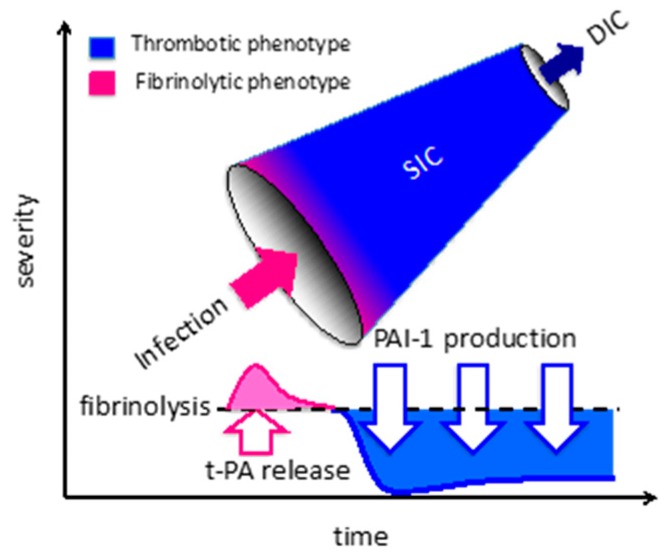
Coagulopathy commonly occurs in sepsis as a critical host response to infection that can progress to disseminated intravascular coagulation (DIC) with an increased mortality. Recent studies have further defined factors responsible for the thromboinflammatory response and intravascular thrombosis, including neutrophil extracellular traps, extracellular vesicles, damage-associated molecular patterns, and endothelial glycocalyx shedding. Diagnosing DIC facilitates sepsis management, and is associated with improved outcomes. Although the International Society on Thrombosis and Haemostasis (ISTH) has proposed criteria for diagnosing overt DIC, these criteria are not suitable for early detection. Accordingly, the ISTH DIC Scientific Standardization Committee has proposed a new category termed "sepsis-induced coagulopathy (SIC)" to facilitate earlier diagnosis of DIC and potentially more rapid interventions in these critically ill patients. Therapy of SIC includes both treatment of the underlying infection and correcting the coagulopathy, with most therapeutic approaches focusing on anticoagulant therapy. Recently, a phase III trial of recombinant thrombomodulin was performed in coagulopathic patients. Although the 28-day mortality was improved by 2.6% (absolute difference), it did not reach statistical significance. However, in patients who met entry criteria for SIC at baseline, the mortality difference was approximately 5% without increased risk of bleeding. In this review, we discuss current advances in managing SIC and DIC.
Keywords: antithrombin; coagulopathy; disseminated intravascular coagulation; sepsis; thrombomodulin.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
