

The effect of CSF drain on the optic nerve in idiopathic intracranial hypertension
- PMID: 31122204
- PMCID: PMC6734439
- DOI: 10.1186/s10194-019-1004-1
The effect of CSF drain on the optic nerve in idiopathic intracranial hypertension
Abstract
Background: Elevation of intracranial pressure in idiopathic intracranial hypertension induces an edema of the prelaminar section of the optic nerve (papilledema). Beside the commonly observed optic nerve sheath distention, information on a potential pathology of the retrolaminar section of the optic nerve and the short-term effect of normalization of intracranial pressure on these abnormalities remains scarce.
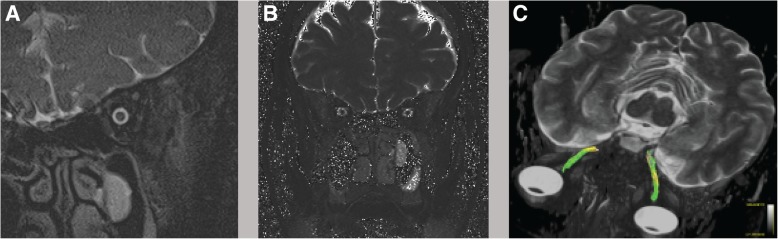
Methods: In this exploratory study 8 patients diagnosed with idiopathic intracranial hypertension underwent a MRI scan (T2 mapping) as well as a diffusion tensor imaging analysis (fractional anisotropy and mean diffusivity). In addition, the clinical presentation of headache and its accompanying symptoms were assessed. Intracranial pressure was then normalized by lumbar puncture and the initial parameters (MRI and clinical features) were re-assessed within 26 h.
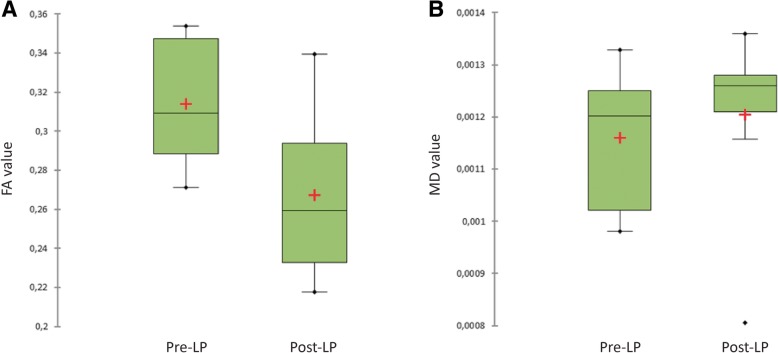
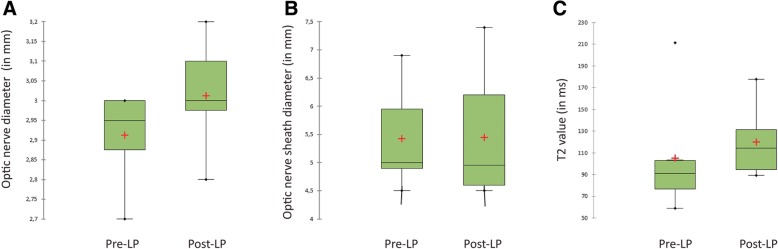
Results: After normalization of CSF pressure, the morphometric MRI scans of the optic nerve and optic nerve sheath remained unchanged. In the diffusion tensor imaging, the fractional anisotropy value was reduced suggesting a tissue decompression of the optic nerve after lumbar puncture. In line with these finding, headache and most of the accompanying symptoms also improved or remitted within that short time frame.
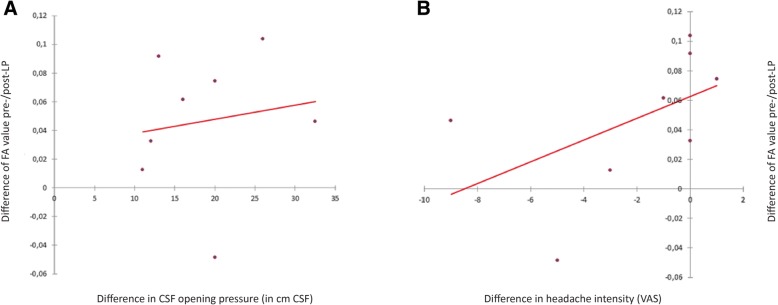
Conclusion: The findings support the hypothesis that the elevation of intracranial pressure induces a microstructural compression of the optic nerve impairing axoplasmic flow and thereby causing the prelaminar papilledema. The microstructural compression of the optic nerve as well as the clinical symptoms improve within hours of normalization of intracranial pressure.
Keywords: DTI; Idiopathic intracranial hypertension; Intracranial pressure; Lumbar puncture; MRI; Optic nerve.
Conflict of interest statement
Jan Hoffmann has consulted for and/or serves on advisory boards for Allergan, Autonomic Technologies Inc. (ATI), Chordate Medical AB, Eli Lilly, Hormosan Pharma, Novartis and Teva. He received honoraria for speaking from Allergan, Autonomic Technologies Inc. (ATI), Chordate Medical AB, Novartis and Teva. These activities are unrelated to the content of this manuscript.
Katharina Maria Kreutz reports no conflict of interest.
Christoph Csapó-Schmidt reports no conflict of interest.
Nils Becker reports no conflict of interest.
Hagen Kunte received personal compensation for speaking from Biogen-Idec, Norvartis, Genzyme, Teva, Merck, Mylan, and Bayer. He also received honoraria for participation in advisory boards from Norvartis, Roche, Genzyme, and Teva as well as travel support to congresses by Norvartis, Genzyme, Teva.
Lucius Samo Fekonja reports no conflict of interest.
Anas Jadan reports no conflict of interest.
Edzard Wiener reports no conflict of interest.
Figures
Similar articles
-
Does IIH Alter Brain Microstructures? - A DTI-Based Approach.Headache. 2017 May;57(5):746-755. doi: 10.1111/head.13039. Epub 2017 Feb 9. Headache. 2017. PMID: 28181232
-
Role of diffusion tensor imaging in the evaluation of white matter integrity in idiopathic intracranial hypertension.Headache. 2024 Oct;64(9):1076-1087. doi: 10.1111/head.14825. Epub 2024 Sep 10. Headache. 2024. PMID: 39257070
-
Optic Nerve Sheath Dilation Is a Possible Marker of CSF Dyshomeostasis in Idiopathic Intracranial Hypertension.Clin Neuroradiol. 2025 Jun;35(2):239-245. doi: 10.1007/s00062-024-01476-2. Epub 2024 Nov 25. Clin Neuroradiol. 2025. PMID: 39585390
-
Complications of Optic Nerve Sheath Fenestration as a Treatment for Idiopathic Intracranial Hypertension.Semin Ophthalmol. 2018;33(1):36-41. doi: 10.1080/08820538.2017.1353810. Semin Ophthalmol. 2018. PMID: 29420144 Review.
-
Pathogenesis of optic disc edema in raised intracranial pressure.Prog Retin Eye Res. 2016 Jan;50:108-44. doi: 10.1016/j.preteyeres.2015.10.001. Prog Retin Eye Res. 2016. PMID: 26453995 Free PMC article. Review.
Cited by
-
Diagnosis and treatment of idiopathic intracranial hypertension.Cephalalgia. 2021 Apr;41(4):472-478. doi: 10.1177/0333102421997093. Epub 2021 Feb 25. Cephalalgia. 2021. PMID: 33631966 Free PMC article. Review.
-
Can optic disc vessel density help in cases of residual disc elevation after shunt surgery in cases of idiopathic intracranial hypertension?Lasers Med Sci. 2024 May 7;39(1):125. doi: 10.1007/s10103-024-04064-5. Lasers Med Sci. 2024. PMID: 38713436 Free PMC article.
-
Which Theory of Cerebrospinal Fluid Production and Absorption Do Neurosurgeons Teach to Medical Students? Survey from Medical Universities in Japan, 2022.Neurol Med Chir (Tokyo). 2024 Jun 15;64(6):241-246. doi: 10.2176/jns-nmc.2023-0277. Epub 2024 May 8. Neurol Med Chir (Tokyo). 2024. PMID: 38719580 Free PMC article.
-
Clinico-radiological correlation of magnetic resonance imaging findings in patients with idiopathic intracranial hypertension.Neuroradiology. 2020 Jan;62(1):49-53. doi: 10.1007/s00234-019-02288-9. Epub 2019 Sep 10. Neuroradiology. 2020. PMID: 31506733
-
Blood pressure lowering enhances cerebrospinal fluid efflux to the systemic circulation primarily via the lymphatic vasculature.Fluids Barriers CNS. 2024 Jan 26;21(1):12. doi: 10.1186/s12987-024-00509-9. Fluids Barriers CNS. 2024. PMID: 38279178 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
