

Type B choledochocele vs duodenal duplication cyst: a diagnostic dilemma and its management: a case report
- PMID: 31122272
- PMCID: PMC6533763
- DOI: 10.1186/s13256-019-2010-2
Type B choledochocele vs duodenal duplication cyst: a diagnostic dilemma and its management: a case report
Abstract
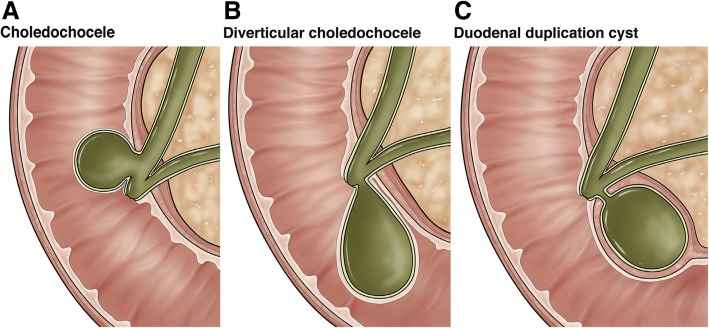
Introduction: Duplication cyst of the alimentary tract is a rare congenital anomaly. Duodenal duplication cyst accounts for less than 5% overall. These entities rarely present in adults. They are often mistaken as choledochoceles. Management is most often complete excision, but it is individualized to the particular case.
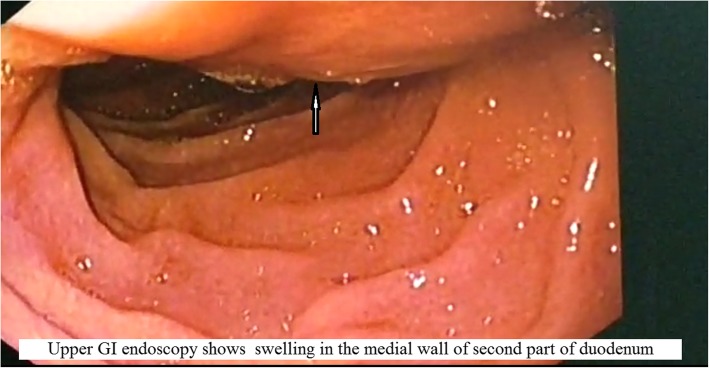
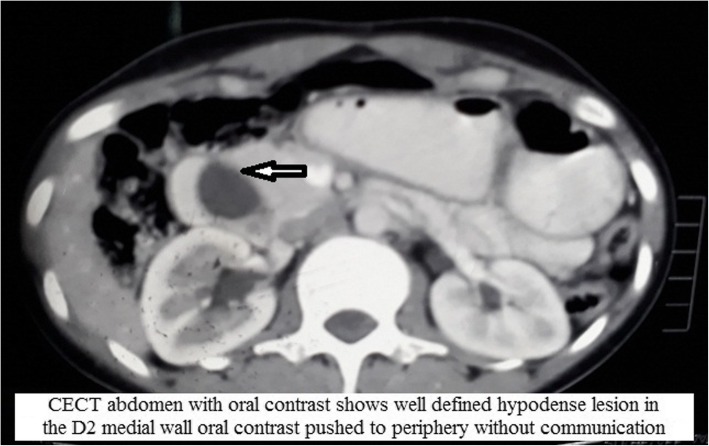
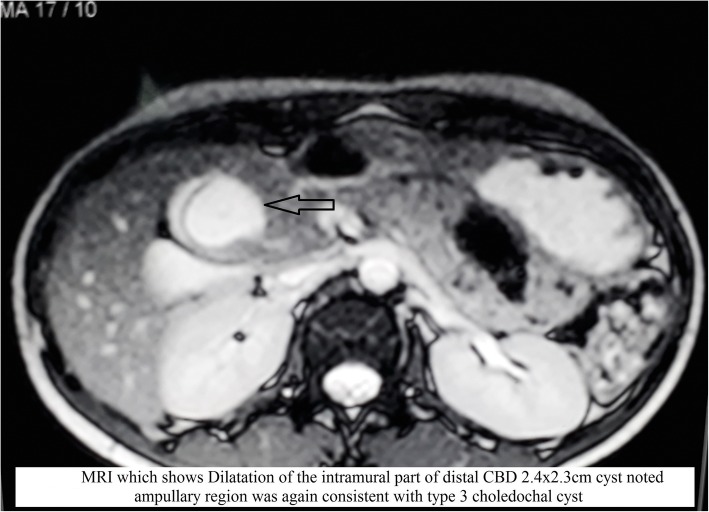
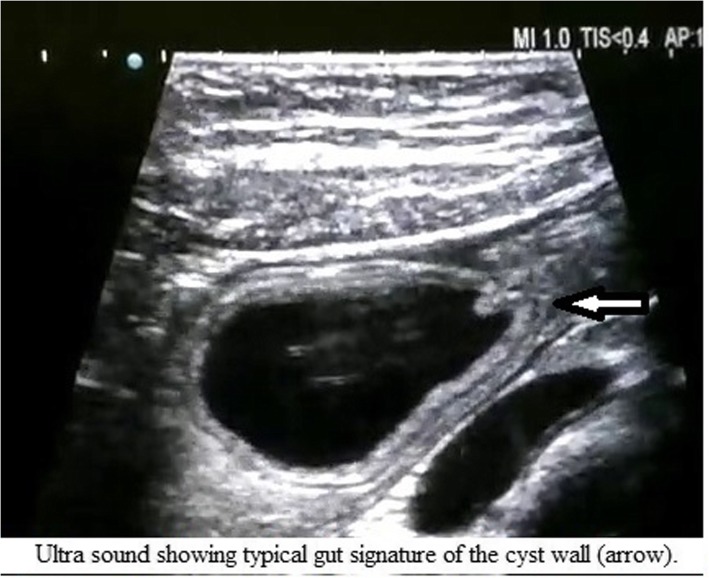
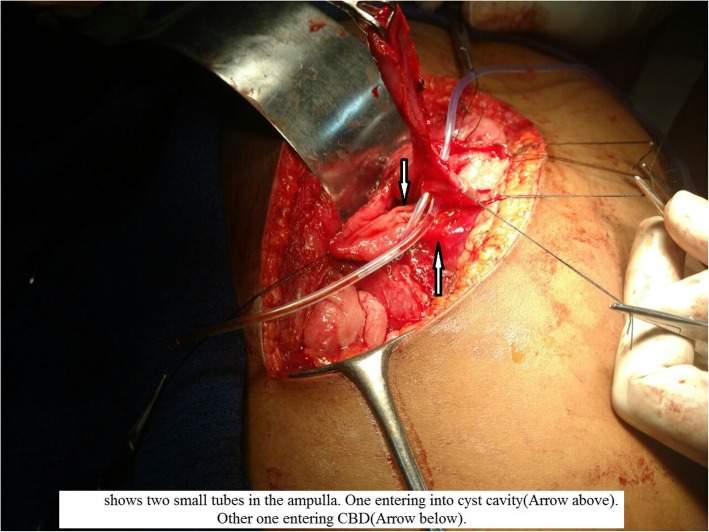
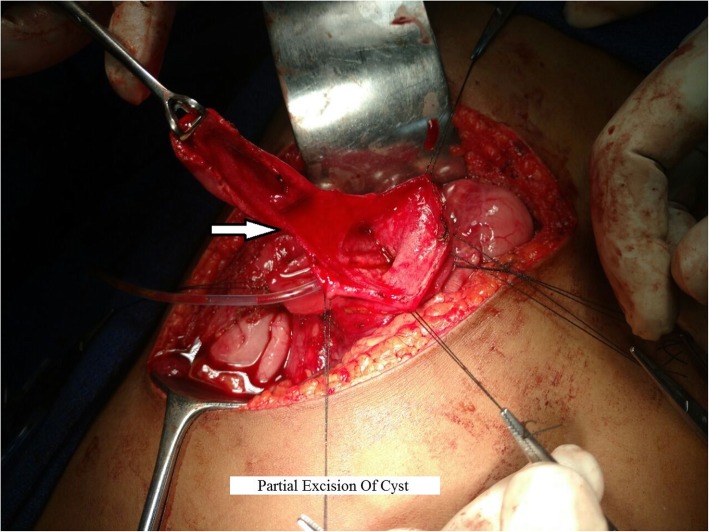
Case presentation: A 22-year-old woman was admitted to our hospital with a history of intermittent colicky right hypochondrial pain not relieved by any medications for the past 3 months. Initially, she was given proton pump inhibitors, but her pain was not relieved. Further evaluation was done, and preoperative imaging showed a cyst in the second part of the duodenum. Magnetic resonance imaging revealed it as a choledochocele, but duodenal duplication cyst was kept in the differential diagnosis. Further ultrasound identified it to be a duplication cyst. After failed endotreatment, the patient was successfully managed with partial excision and marsupialization.
Conclusion: Duodenal duplication cyst is uncommon and rarely diagnosed in adults. Duplications in the duodenum should always be a part of the differential diagnosis, especially in cystic lesions. Ultrasonogram of the cyst might lead to the proper diagnosis. Surgery is the treatment of choice if endotherapy is not successful.
Keywords: Ampulla; Case report; Choledochocele; Duplication cyst; Gut signature; Marsupialization.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Periampullary duodenal duplication cyst masquerading as a choledochocele.Pediatr Surg Int. 2012 Oct;28(10):1035-9. doi: 10.1007/s00383-012-3116-4. Epub 2012 Jul 1. Pediatr Surg Int. 2012. PMID: 22752148
-
Duodenal duplication cyst: a potentially malignant disease.Ann Surg Oncol. 2012 Nov;19(12):3753-4. doi: 10.1245/s10434-012-2502-4. Epub 2012 Jul 26. Ann Surg Oncol. 2012. PMID: 22832999
-
[Endoscopic treatment of duodenal duplication cyst].Khirurgiia (Mosk). 2021;(3):66-69. doi: 10.17116/hirurgia202103166. Khirurgiia (Mosk). 2021. PMID: 33710829 Russian.
-
Choledochocele--a rare cause of necrotising pancreatitis in childhood.Eur J Pediatr Surg. 2000 Aug;10(4):258-64. doi: 10.1055/s-2008-1072370. Eur J Pediatr Surg. 2000. PMID: 11034517 Review.
-
Diagnosis and treatment of choledochoceles.Clin Gastroenterol Hepatol. 2014 Feb;12(2):196-203. doi: 10.1016/j.cgh.2013.04.037. Epub 2013 May 6. Clin Gastroenterol Hepatol. 2014. PMID: 23660418 Review.
References
-
- Deftereos S, Soultanidis H, Limas C, Tsalkidis A, Gouliamtzi E, Manavis J. Duodenal duplication. Is ultrasound appearance enough to confirm the diagnosis. Rom J Gastroenterol. 2004;13:345–347. - PubMed
-
- Guerra L, Greco F, Di Matteo F, Pandolfi M, Taffon C, Zobel BB. Duodenal duplication cyst: a rare case report. Indian J Case Rep. 2016;2(3):62–65.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
