

Etanercept treatment for extended oligoarticular juvenile idiopathic arthritis, enthesitis-related arthritis, or psoriatic arthritis: 6-year efficacy and safety data from an open-label trial
- PMID: 31122296
- PMCID: PMC6533709
- DOI: 10.1186/s13075-019-1916-9
Etanercept treatment for extended oligoarticular juvenile idiopathic arthritis, enthesitis-related arthritis, or psoriatic arthritis: 6-year efficacy and safety data from an open-label trial
Abstract
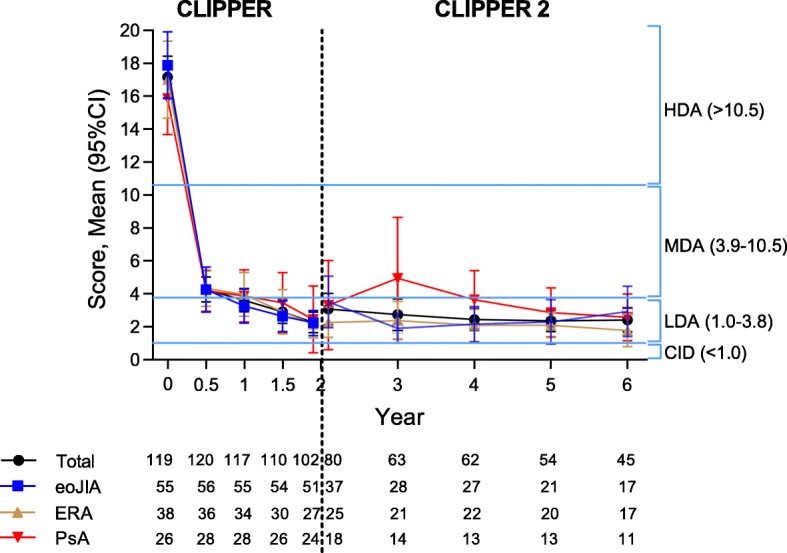
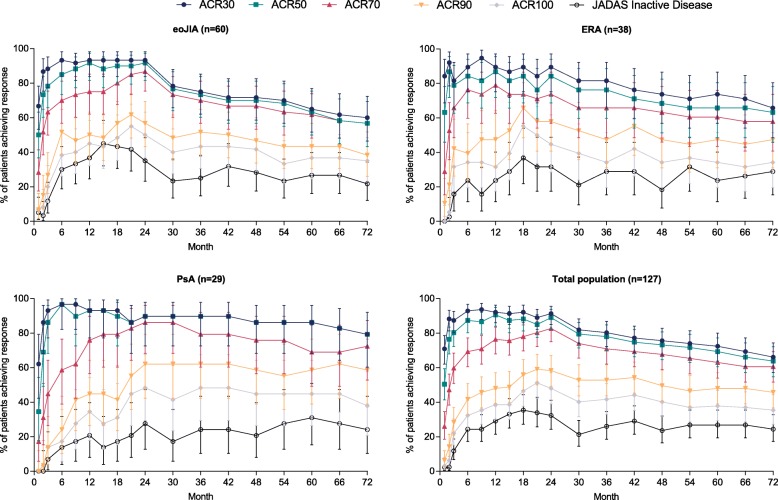
Background: To describe the 6-year safety and efficacy of etanercept (ETN) in children with extended oligoarticular juvenile idiopathic arthritis (eoJIA), enthesitis-related arthritis (ERA), and psoriatic arthritis (PsA) METHODS: Patients who completed the 2-year, open-label, phase III CLinical Study In Pediatric Patients of Etanercept for Treatment of ERA, PsA, and Extended Oligoarthritis (CLIPPER) were allowed to enroll in its 8-year long-term extension (CLIPPER2). Children received ETN at a once-weekly dose of 0.8 mg/kg, up to a maximum dose of 50 mg/week. Efficacy assessments included the JIA core set of outcomes, the JIA American College of Rheumatology response criteria (JIA-ACR), and the Juvenile Arthritis Disease Activity Score (JADAS). Efficacy data are reported as responder analyses using a hybrid method for missing data imputation and as observed cases. Safety assessments included treatment-emergent adverse events (TEAEs).
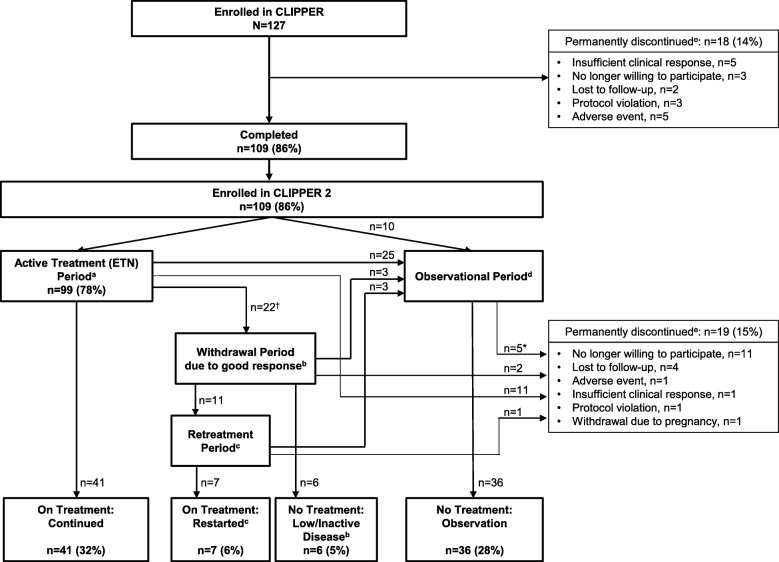
Results: Out of 127 patients originally enrolled in CLIPPER, 109 (86%) entered CLIPPER2. After 6 years of trial participation (2 years in CLIPPER and 4 years in CLIPPER2), 41 (32%) patients were still taking ETN, 13 (11%) entered the treatment withdrawal phase after achieving low/inactive disease (of whom 7 had to restart ETN), 36 (28%) discontinued treatment for other reasons but are still being observed, and 37 (29%) discontinued treatment permanently. According to the hybrid imputation analysis, proportions of patients achieving JIA ACR90, JIA ACR100, and JADAS inactive disease after the initial 2 years of treatment were 58%, 48%, and 32%, respectively. After the additional 4 years, those proportions in patients who remained in the trial were 46%, 35%, and 24%. Most frequently reported TEAEs [n (%), events per 100 patient-years] were headache [28 (22%), 5.3], arthralgia [24 (19%), 4.6], and pyrexia [20 (16%), 3.8]. Number and frequency of TEAEs, excluding infections and injection site reactions, decreased over the 6-year period from 193 and 173.8, respectively, during year 1 to 37 and 61.3 during year 6. A single case of malignancy (Hodgkin's lymphoma) and no cases of active tuberculosis, demyelinating disorders, or deaths were reported.
Conclusions: Open-label etanercept treatment for up to 6 years was safe, well tolerated, and effective in patients with eoJIA, ERA, and PsA.
Trial registration: ClinicalTrials.gov: CLIPPER, NCT00962741 , registered 20 August, 2009, CLIPPER2, NCT01421069 , registered 22 August, 2011.
Keywords: Clinical trial; Efficacy; Enthesitis-related arthritis; Enthesitis-related arthritis (ERA); Etanercept; Extended oligoarticular juvenile idiopathic arthritis (eoJIA); Juvenile idiopathic arthritis; Psoriatic arthritis (PsA); Safety.
Conflict of interest statement
I. Foeldvari has served on advisory boards with AbbVie, Novartis, Chugai, and Genzyme.
T. Constantin has received speaker’s fees from or served as a consultant for AbbVie, Novartis, Pfizer, and Roche.
J. Vojinović has received honoraria from AbbVie, Pfizer, TEVA, MSD, and Roche.
G. Horneff has received honoraria from Chugai, UCB, Pfizer, AbbVie, Roche, and Novartis.
J. Dehoorne has received speaker’s fees from or served as a consultant for AbbVie, Pfizer, and Roche.
V. Stanevicha has received consulting fees from AbbVie and Roche and has a partnership with Pfizer.
I. Nikishina has received honoraria from AbbVie, Bristol-Myers Squibb, Janssen, MSD, Novartis, Pfizer, and Roche.
P. Doležalová has received speaker’s bureau honoraria from Pfizer, AbbVie, Novartis, Hoffman-La Roche, Medac, Swedish Orphan Biovitrum, Eli Lilly, Sanofi, and Genzyme.
R. Pedersen and B. Vlahos are employees of Pfizer, the sponsor of this study, and own company stock.
J. Bukowski is a former employee of Pfizer, the sponsor of this study, and may own company stock.
A. Martini has received speaker’s bureau and honoraria from Abbott, AbbVie, Amgen, Biogen Idec, Bristol-Myers Squibb, Astellas, Boehringer, Italfarmaco, Janssen, MedImmune, Novartis, Novo Nordisk, Pfizer, Sanofi, Roche, Servier, and Takeda.
N. Ruperto has received speaker’s bureau and honoraria from Abbott, AbbVie, Amgen, Biogen Idec, Astellas, Alter, AstraZeneca, Boehringer, Bristol-Myers Squibb, CD-Pharma, Celgene, Crescendo Bioscience, EMD Serono, Hoffman-La Roche, Italfarmaco, Janssen, MedImmune, Medac, Novartis, Novo Nordisk, Pfizer, Sanofi Aventis, Servier, Takeda, and Vertex.
The IRCCS Istituto Giannina Gaslini, which is the public hospital where Dr. Ruperto and Prof Martini work as full-time employees, has received contributions to support the research activities of the network of PRINTO (
V. Chasnyk, V. Panaviene, G. Sušić, K. Kobusinska, Z. Zuber, B. Dobrzyniecka, B. Bader-Meunier, L. Breda, C. Job-Deslandre, I. Rumba-Rozenfelde, and N. Wulffraat declare that they have no competing interests.
Figures
References
-
- Petty RE, Southwood TR, Manners P, Baum J, Glass DN, Goldenberg J, He X, Maldonado-Cocco J, Orozco-Alcala J, Prieur AM, et al. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004;31(2):390–392. - PubMed
-
- Brunner HI, Ruperto N, Tzaribachev N, Horneff G, Chasnyk VG, Panaviene V, Abud-Mendoza C, Reiff A, Alexeeva E, Rubio-Perez N, et al. Subcutaneous golimumab for children with active polyarticular-course juvenile idiopathic arthritis: results of a multicentre, double-blind, randomised-withdrawal trial. Ann Rheum Dis. 2018;77(1):21–29. doi: 10.1136/annrheumdis-2016-210456. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
