

Biliary Involvement in Type 2 Autoimmune Pancreatitis
- PMID: 31123447
- PMCID: PMC6514518
- DOI: 10.1159/000499422
Biliary Involvement in Type 2 Autoimmune Pancreatitis
Abstract
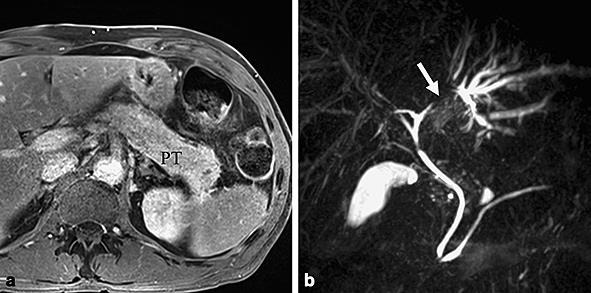
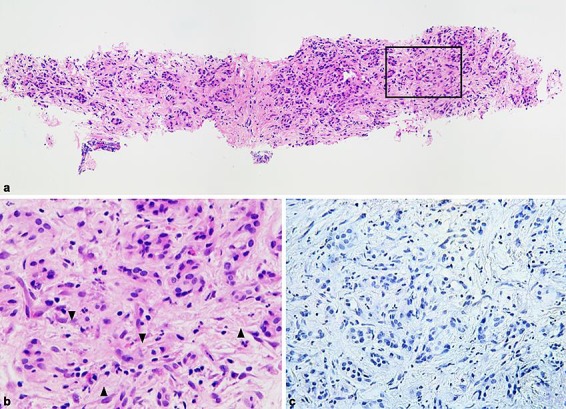
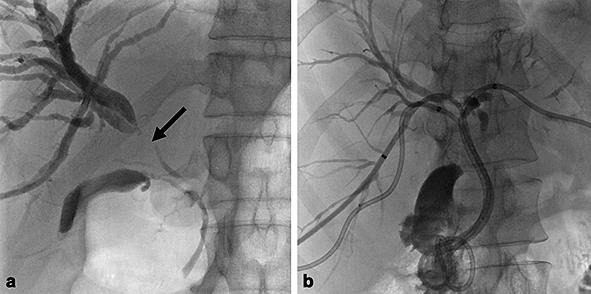
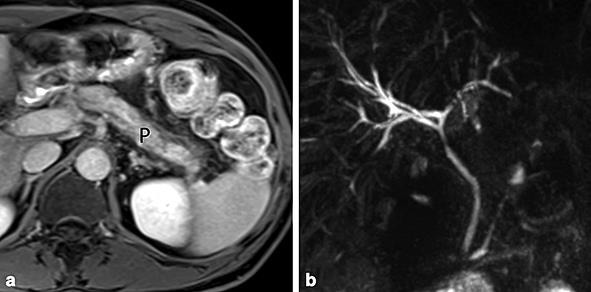
Autoimmune pancreatitis (AIP) is a rare condition classified in 2 subtypes. Their distinction relies on a combination of clinical, serological, morphological and histological features. Type 1 is a pancreatic manifestation of IgG4-related disease characterized by multiorgan infiltration by IgG4 plasmocytes. In this condition, hepatobiliary infiltration is frequent and often mimics cholangiocarcinoma or primary sclerosing cholangitis. On the other hand, type 2 is commonly limited to the pancreas. Herein, we describe the case of a patient who presented a type 2 AIP associated with cholangiopathy, a condition not described in the established criteria. He first developed a pancreatitis identified as type 2 by the typical histopathological features and lack of IgG4 in the serum and tissue. Despite a good clinical response to steroids, cholestasis persisted, identified by MR cholangiography as a stricture of the left hepatic duct with dilatation of the intrahepatic bile duct in segments 2 and 3. Biliary cytology was negative. Evolution was favorable but after steroid tapering a few months later, the patient suffered from recurrence of the pancreatitis as well as progression of biliary attempt, suspicious for cholangiocarcinoma. As the investigations again ruled out neoplastic infiltration or primary sclerosing cholangitis, azathioprine was initiated with resolution of both pancreatic and biliary attempts.
Keywords: Autoimmune pancreatitis; Biliary involvement.
Figures
References
-
- Shimosegawa T, Chari ST, Frulloni L, Kamisawa T, Kawa S, Mino-Kenudson M, et al. International Association of Pancreatology International consensus diagnostic criteria for autoimmune pancreatitis: guidelines of the International Association of Pancreatology. Pancreas. 2011 Apr;40((3)):352–8. - PubMed
-
- Okazaki K, Chari ST, Frulloni L, Lerch MM, Kamisawa T, Kawa S, et al. International consensus for the treatment of autoimmune pancreatitis. Pancreatology. 2017 Jan-Feb;17((1)):1–6. - PubMed
-
- Lorenzo D, Maire F, Stefanescu C, Gornet JM, Seksik P, Serrero M, et al. Features of Autoimmune Pancreatitis Associated with Inflammatory Bowel Diseases. Clin Gastroenterol Hepatol. 2017 - PubMed
-
- Geary K, Yazici C, Seibold A, Guzman G. IgG4-Related Cholangiopathy and Its Mimickers: A Case Report and Review Highlighting the Importance of Early Diagnosis. Int J Surg Pathol. 2018 Apr;26((2)):165–73. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
