

Alternatives to Rapid Sequence Intubation: Contemporary Airway Management with Ketamine
- PMID: 31123547
- PMCID: PMC6526883
- DOI: 10.5811/westjem.2019.4.42753
Alternatives to Rapid Sequence Intubation: Contemporary Airway Management with Ketamine
Abstract
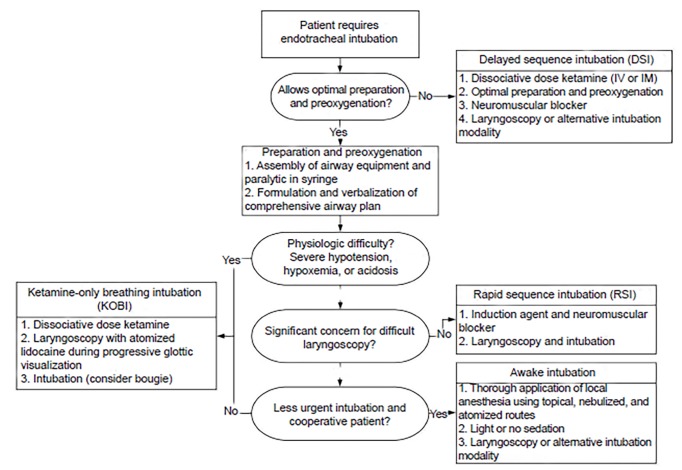
Endotracheal intubation (ETI) is a high-risk procedure commonly performed in emergency medicine, critical care, and the prehospital setting. Traditional rapid sequence intubation (RSI), the simultaneous administration of an induction agent and muscle relaxant, is more likely to harm patients who do not allow appropriate preparation and preoxygenation, have concerning airway anatomy, or severe hypoxia, acidemia, or hypotension. Ketamine, a dissociative anesthetic, can be used to facilitate two alternatives to RSI to augment airway safety in these scenarios: delayed sequence intubation - the use of ketamine to allow airway preparation and preoxygenation in the agitated patient; and ketamine-only breathing intubation, in which ketamine is used without a paralytic to facilitate ETI as the patient continues to breathe spontaneously. Ketamine may also provide hemodynamic benefits during standard RSI and is a valuable agent for post-intubation analgesia and sedation. When RSI is not an optimal airway management strategy, ketamine's unique pharmacology can be harnessed to facilitate alternative approaches that may increase patient safety.
Conflict of interest statement
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. No author has professional or financial relationships with any companies that are relevant to this study. There are no conflicts of interest or sources of funding to declare.
Figures
Comment in
-
Ketamine as Monotherapy in Difficult Airways Is Not Ready for Prime Time.West J Emerg Med. 2019 Oct 17;20(6):970-971. doi: 10.5811/westjem.2019.8.43881. West J Emerg Med. 2019. PMID: 31738726 Free PMC article. No abstract available.
References
-
- Cook TM, MacDougall-Davis SR. Complications and failure of airway management. Br J Anaesth. 2012;109(Suppl 1):i68–i85. - PubMed
-
- Ko BS, Ahn R, Ryoo SM, et al. Prevalence and outcomes of endotracheal intubation–related cardiac arrest in the ED. Am J Emerg Med. 2015;33(11):1642–5. - PubMed
-
- Mort TC. Complications of emergency tracheal intubation: hemodynamic alterations - part I. J Intensive Care Med. 2007;22(3):157–65. - PubMed
-
- Heffner AC, Swords DS, Neale MN, et al. Incidence and factors associated with cardiac arrest complicating emergency airway management. Resuscitation. 2013;84(11):1500–4. - PubMed