

Availability of Bedside and Laboratory Testing for Carbon Monoxide Poisoning in the Upper Midwestern United States
- PMID: 31123553
- PMCID: PMC6526886
- DOI: 10.5811/westjem.2019.2.41428
Availability of Bedside and Laboratory Testing for Carbon Monoxide Poisoning in the Upper Midwestern United States
Abstract
Introduction: The objective of this study was to assess the ability to test patients for carbon monoxide (CO) exposure in all hospitals in three United States (U.S.) Midwestern states.
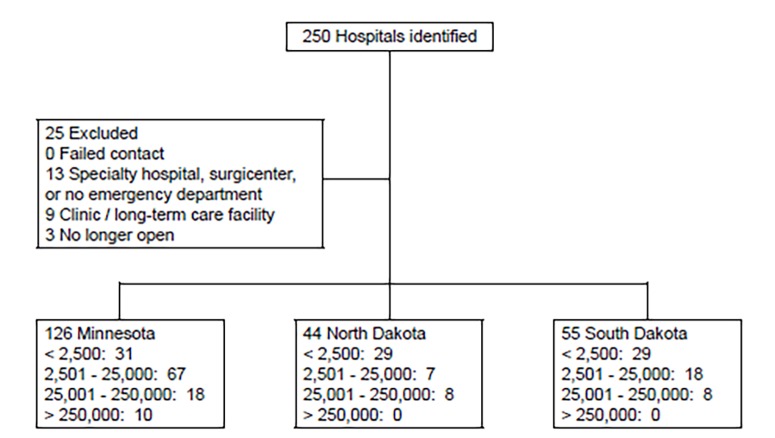
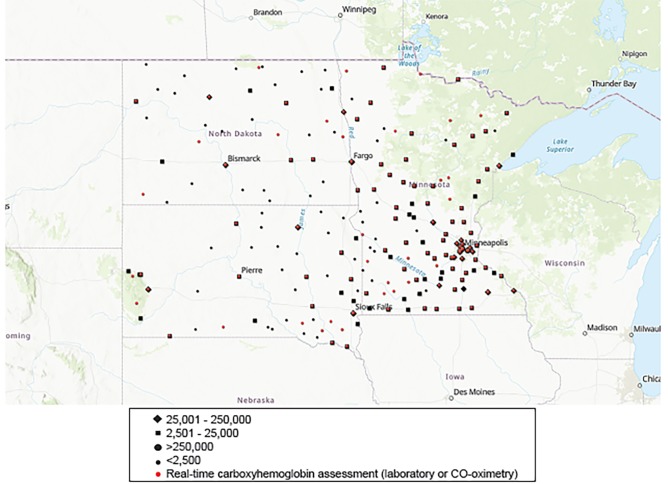
Methods: We surveyed hospitals in three states. Telephone queries assessed processes for measuring carboxyhemoglobin, including capacity for real-time vs send-out testing. Facilities were separated based on their location's population size for further analysis. Descriptive statistics are reported.
Results: Of the 250 hospitals queried, we ultimately excluded 25. Nearly all (220, 97.8%) reported a process in place to test for CO exposure. Over 40% (n=92) lacked real-time testing. Testing ability was positively associated with increasing population size quartile (range 32.6% - 100%). Hospitals in the lowest-quartile population centers were more likely to report that they were unable to test in real time than those in the largest-quartile population centers (67.4% vs 0%).
Conclusion: In a large geographic region encompassing three states, hospital-based and real-time capacity to test for CO exposure is not universal. Hospitals in smaller population areas are more likely to lack real-time testing or any testing at all. This may have significant public health, triage, and referral implications for patients.
Conflict of interest statement
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. No author has professional or financial relationships with any companies that are relevant to this study. There are no conflicts of interest or sources of funding to declare.
Figures
Similar articles
-
Carboxyhemoglobin measurement by hospitals: implications for the diagnosis of carbon monoxide poisoning.J Emerg Med. 2006 Jul;31(1):13-6. doi: 10.1016/j.jemermed.2005.09.010. J Emerg Med. 2006. PMID: 16798147
-
Variability in hyperbaric oxygen treatment for acute carbon monoxide poisoning.Undersea Hyperb Med. 2012 Mar-Apr;39(2):627-38. Undersea Hyperb Med. 2012. PMID: 22530446
-
Carbon monoxide poisoning. An occult epidemic.Postgrad Med. 1992 Sep 15;92(4):86-8, 92-6. doi: 10.1080/00325481.1992.11701467. Postgrad Med. 1992. PMID: 1528817 Review.
-
Diagnostic Performance of Carbon Monoxide Testing by Pulse Oximetry in the Emergency Department.Respir Care. 2019 Nov;64(11):1351-1357. doi: 10.4187/respcare.06365. Epub 2019 Apr 30. Respir Care. 2019. PMID: 31040204
-
Carbon monoxide poisoning.Crit Care Clin. 2012 Oct;28(4):537-48. doi: 10.1016/j.ccc.2012.07.007. Crit Care Clin. 2012. PMID: 22998990 Review.
References
-
- Raub JA, Mathieu-Nolf M, Hampson NB, et al. Carbon monoxide poisoning - a public health perspective. Toxicology. 2000;145(1):1–14. - PubMed
-
- Hampson NB, Weaver LK. Carbon monoxide poisoning: a new incidence for an old disease. Undersea Hyperb Med. 2007;34(3):163–8. - PubMed
-
- Hampson NB. U.S. mortality due to carbon monoxide poisoning, 1999–2014. Accidental and intentional deaths. Ann Am Thorac Soc. 2016;13(10):1768–74. - PubMed