

Constitutive alterations in vesicular trafficking increase the sensitivity of cells from celiac disease patients to gliadin
- PMID: 31123714
- PMCID: PMC6527696
- DOI: 10.1038/s42003-019-0443-1
Constitutive alterations in vesicular trafficking increase the sensitivity of cells from celiac disease patients to gliadin
Erratum in
-
Author Correction: Constitutive alterations in vesicular trafficking increase the sensitivity of cells from celiac disease patients to gliadin.Commun Biol. 2020 Apr 2;3(1):166. doi: 10.1038/s42003-020-0906-4. Commun Biol. 2020. PMID: 32242079 Free PMC article.
Abstract
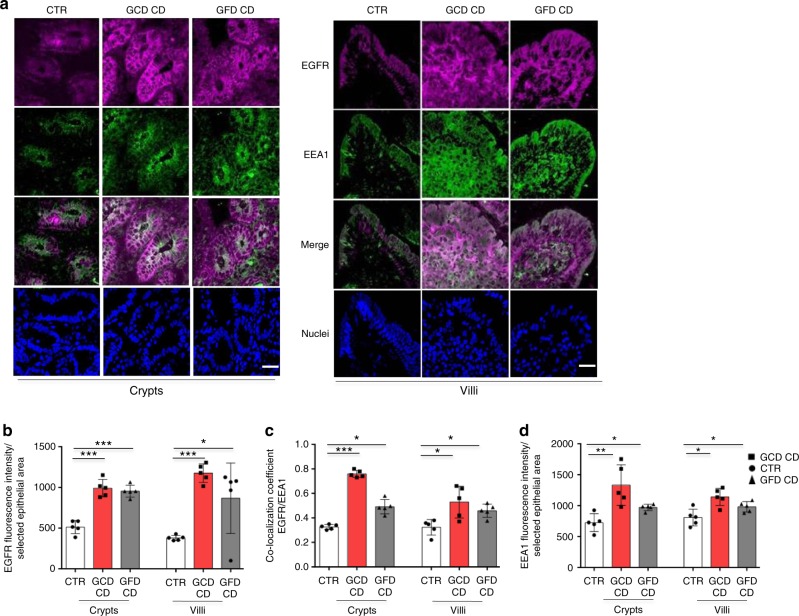
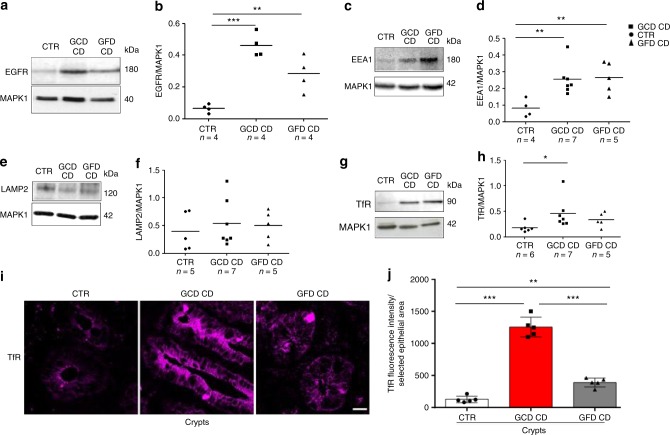
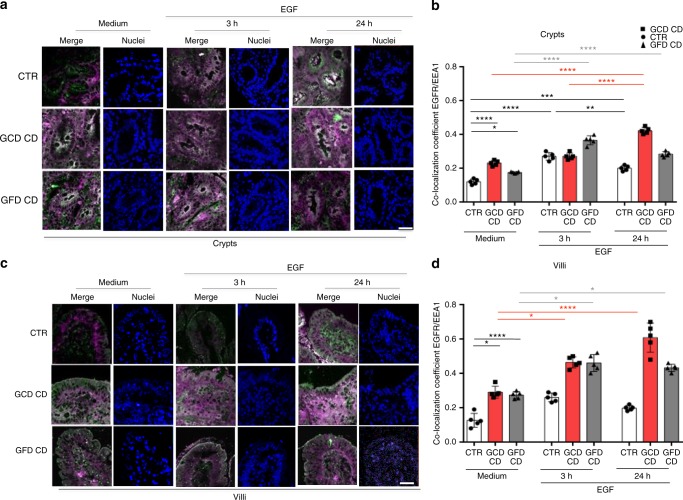
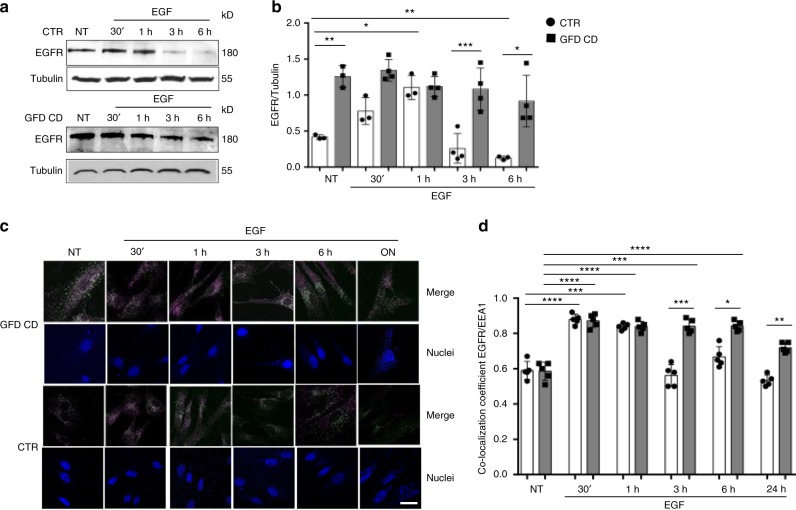
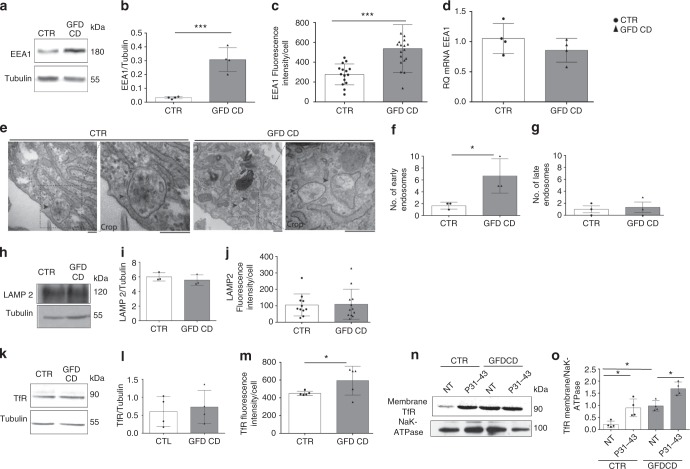
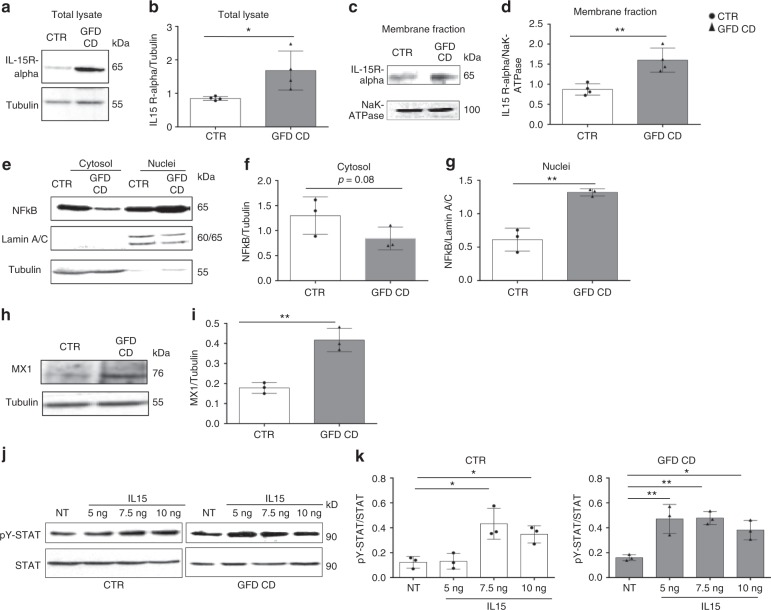
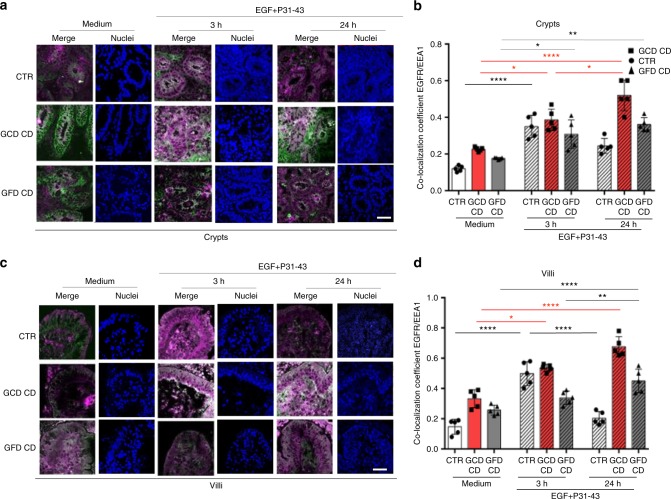
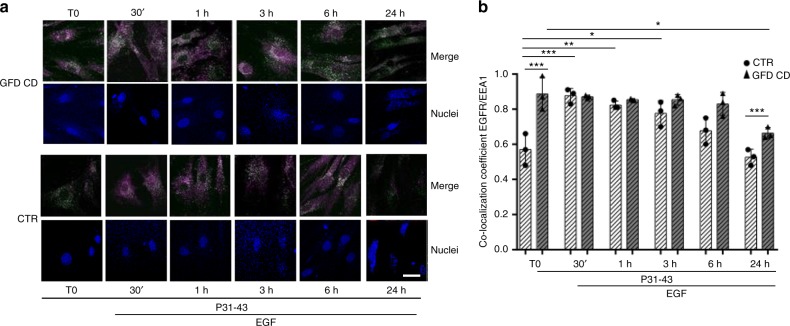
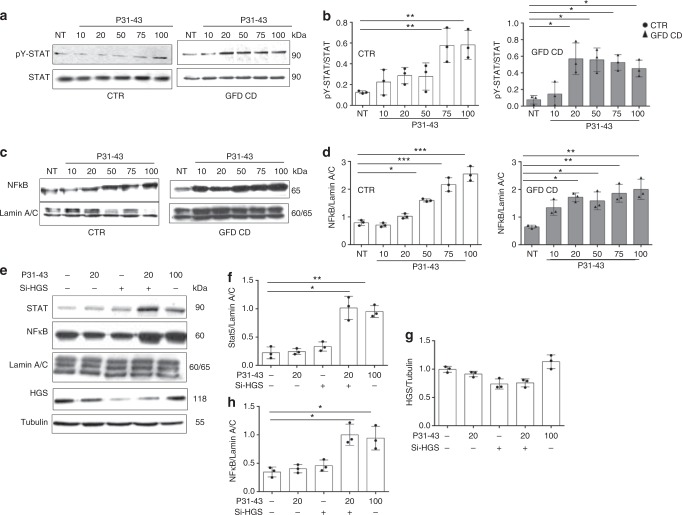
Celiac Disease (CD) is an autoimmune disease characterized by inflammation of the intestinal mucosa due to an immune response to wheat gliadins. Some gliadin peptides (e.g., A-gliadin P57-68) induce an adaptive Th1 pro-inflammatory response. Other gliadin peptides (e.g., A-gliadin P31-43) induce a stress/innate immune response involving interleukin 15 (IL15) and interferon α (IFN-α). In the present study, we describe a stressed/inflamed celiac cellular phenotype in enterocytes and fibroblasts probably due to an alteration in the early-recycling endosomal system. Celiac cells are more sensitive to the gliadin peptide P31-43 and IL15 than controls. This phenotype is reproduced in control cells by inducing a delay in early vesicular trafficking. This constitutive lesion might mediate the stress/innate immune response to gliadin, which can be one of the triggers of the gliadin-specific T-cell response.
Keywords: Coeliac disease; Endosomes.
Conflict of interest statement
Competing interestsThe authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
