

Chordoma located in the jugular foramen: Case report
- PMID: 31124949
- PMCID: PMC6571403
- DOI: 10.1097/MD.0000000000015713
Chordoma located in the jugular foramen: Case report
Abstract
Rationale: Chordomas are rare malignant neoplasms arised from residual embryonic notochordal tissue, mostly located in the axial midline. Tumors along extra-axial locations in the head and neck are rare. Chordomas located in the jugular foramen are extremely rare, with a low incidence of 0.2%.
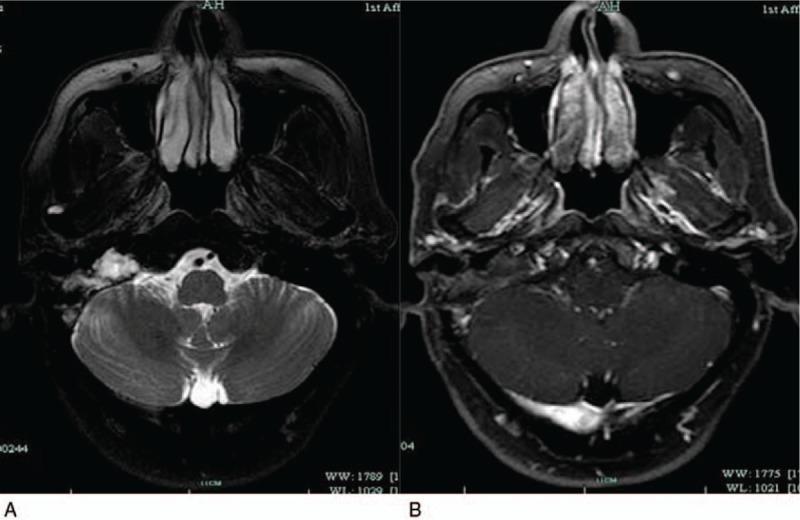
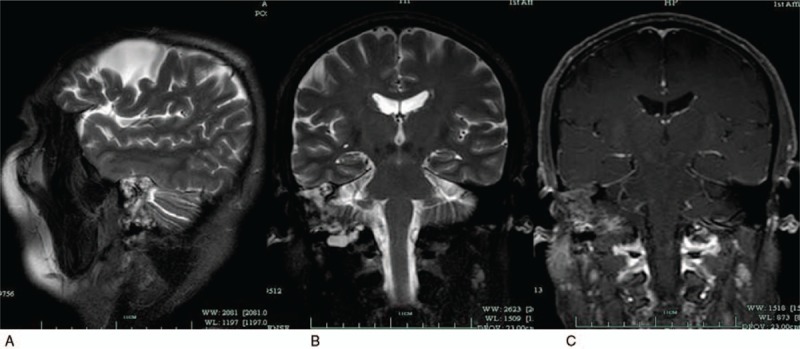
Patient concerns: A 64-year-old male with 20 years of dizziness history complaining of 6 months of severe dizziness: significant with the changing of the body posture, vertigo which can be self-remissioned within 1 minute and hearing loss of both ears, without headache, nausea, dysphagia, or otalgia. Computed tomography and magnetic resonance imaging (MRI) were performed before surgery which suggests various possibilities. Immunohistochemistry helped to confirm the final diagnosis.
Diagnoses: Immunohistochemistry demonstrated diffuse positivity for S100 (+++), positivity for D2-40 (focal +), EMA (+), and PR (+). Ki-67 labeling index was estimated at 2% focally. The final diagnosis was chordoma.
Interventions: The tumor was excised via retro-sigmoid approach without postoperative radiotherapy.
Outcomes: Facial paralysis occurred in this case. House-Brackmann facial nerve grading system was used to evaluate the facial paralysis of this patient. It is considered as H-B grade IV. The patient was followed up regularly every month after operation, totally for 9 months. An MRI of the brain was performed 6 months after surgery which shows a small range of abnormal signals similar to the previous MRI in the jugular foramen, suggesting that there may be residual or recurrent tumor. And facial paralysis stays at H-B grade IV without any recovery.
Lessons: It is a big challenge for us to remove giant tumors located in the jugular foramen because of its unique anatomy. Access should be combined with retro-sigmoid or infra-temporal fossa approach to remove such tumors. Chordomas is a malignant neoplasm which may need radiotherapy after surgery, particularly those with subtotal and partial resection.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures





References
-
- Dwivedi RC, Ojha BK, Mishra A, et al. A rare case of jugular foramen chordoma with an unusual extension. Arch Otolaryngol Head Neck Surg 2011;137:513–6. - PubMed
-
- Stemple DL. Structure and function of the notochord: an essential organ for chordate development. Development (Cambridge, England) 2005;132:2503–12. - PubMed
-
- Tirabosco R, Mangham DC, Rosenberg AE, et al. Brachyury expression in extra-axial skeletal and soft tissue chordomas: a marker that distinguishes chordoma from mixed tumor/myoepithelioma/parachordoma in soft tissue. Am J Surg Pathol 2008;32:572–80. - PubMed
-
- Erdem E, Angtuaco EC, Van Hemert R, et al. Comprehensive review of intracranial chordoma. Radiographics 2003;23:995–1009. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
