

Efficacy of Mindfulness-Based Cognitive Training in Surgery: Additional Analysis of the Mindful Surgeon Pilot Randomized Clinical Trial
- PMID: 31125095
- PMCID: PMC6632137
- DOI: 10.1001/jamanetworkopen.2019.4108
Efficacy of Mindfulness-Based Cognitive Training in Surgery: Additional Analysis of the Mindful Surgeon Pilot Randomized Clinical Trial
Abstract
Importance: Mindfulness meditation training has been shown to be feasible in surgical trainees, but affective, cognitive, and performance benefits seen in other high-stress populations have yet to be evaluated.
Objective: To explore potential benefits to stress, cognition, and performance in postgraduate year 1 (PGY-1) surgery residents receiving modified mindfulness-based stress reduction (modMBSR).
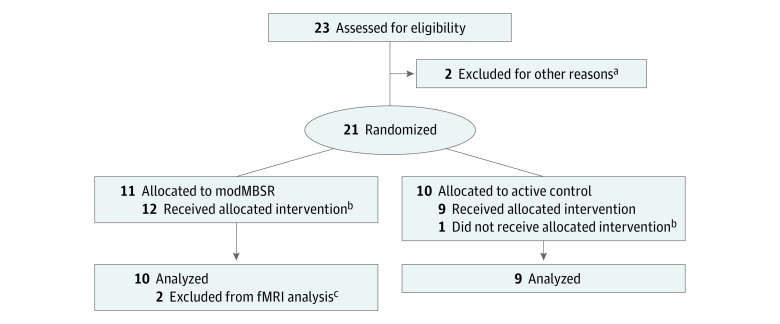
Design, setting, and participants: This follow-up study is an analysis of the Mindful Surgeon pilot randomized clinical trial of modMBSR (n = 12) vs an active control (n = 9), evaluated at baseline (T1), postintervention (T2), and 1 year (T3), took place at an academic medical center residency training program among PGY-1 surgery residents. Data were collected between June 2016 and June 2017 and analyzed from June 2017 to December 2017.
Interventions: Weekly 2-hour modMBSR classes and 20 minutes of daily home practice during an 8-week period vs an active control (different content, same structure).
Main outcomes and measures: Preliminary evidence of efficacy was explored, primarily focusing on perceived stress and executive function and secondarily on burnout, depression, motor skill performance, and changes in blood oxygen level-dependent functional neuroimaging during an emotion regulation task. Group mean scores were calculated at T1, T2, and T3 and in linear mixed-effects multivariate analysis. Effect size for analysis of covariance is presented as partial η2 with the following cutoff points: small, less than 0.06; medium, 0.06 to 0.14; large, greater than 0.14.
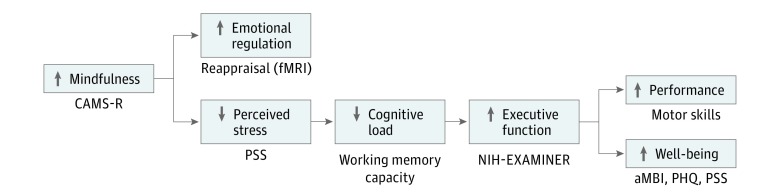
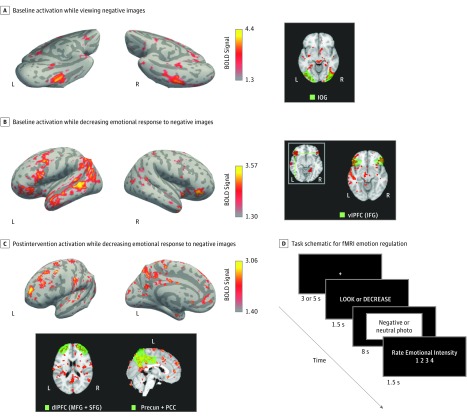
Results: Postgraduate year 1 surgery residents (N = 21; 8 [38%] women) were randomized to a modMBSR arm (n = 12) or an active control arm (n = 9). Linear mixed-effects modeling revealed differences at T2 and T3 in perceived stress (mean [SD] difference at T2: modMBSR, 1.42 [5.74]; control, 3.44 [6.71]; η2 = 0.07; mean [SD] difference at T3: modMBSR, 1.00 [4.18]; control, 1.33 [4.69]; η2 = 0.09) and in mindfulness (mean [SD] difference at T2: modMBSR, 3.08 [3.63]; control, 1.56 [4.28]; η2 = 0.13; mean [SD] difference at T3: modMBSR, 2.17 [3.66]; control, -0.11 [6.19]; η2 = 0.15). Burnout at T2 (mean [SD] difference: modMBSR, 4.50 [9.08]; control, 3.44 [6.71]; η2 = 0.01) and T3 (mean [SD] difference: modMBSR, 5.50 [9.96]; control, 5.56 [9.69]; η2 = 0.01) showed similar increase in both groups. Working memory increased more at T2 in the modMBSR arm (mean [SD] difference, 0.35 [0.60]) than in the control arm (mean [SD] difference, 0.21 [0.74]; η2 = 0.02) and at T3 (modMBSR, 0.68 [0.69]; control, 0.26 [0.58]; η2 = 0.20). Cognitive control decreased more in the control arm at T2 (mean [SD] difference at T2: modMBSR, 0.15 [0.40]; control, -0.07 [0.32]; η2 = 0.13) and at T3 (mean [SD] difference: modMBSR, 0.07 [0.59]; control, -0.26 [0.53]; η2 = 0.16). Mean (SD) circle-cutting time improved more at T2 in the modMBSR arm (-24.08 [63.00] seconds) than in the control arm (-4.22 [112.94] seconds; η2 = 0.23) and at T3 in the modMBSR arm (-4.83 [77.94] seconds) than in the control arm (11.67 [145.17] seconds; η2 = 0.13). Blood oxygen level-dependent functional neuroimaging during an emotional regulation task showed unique postintervention activity in the modMBSR arm in areas associated with executive function control (dorsolateral prefrontal cortex) and self-awareness (precuneus).
Conclusions and relevance: In this pilot randomized clinical trial, modMBSR in PGY-1 surgery residents showed potential benefits to well-being and executive function, suggesting a powerful role for mindfulness-based cognitive training to support resident well-being and performance, as mandated by the Accreditation Council for Graduate Medical Education.
Trial registration: ClinicalTrials.gov identifier: NCT03141190.
Conflict of interest statement
Figures
Comment in
-
Mindfulness-Based Training Improves Technical Skills and Emotional Regulation for Surgical Residents.JAMA Netw Open. 2019 May 3;2(5):e194087. doi: 10.1001/jamanetworkopen.2019.4087. JAMA Netw Open. 2019. PMID: 31125093 No abstract available.
