

Risk Factors Associated With Atrioventricular Block
- PMID: 31125096
- PMCID: PMC6632153
- DOI: 10.1001/jamanetworkopen.2019.4176
Risk Factors Associated With Atrioventricular Block
Abstract
Importance: Pacemaker implantations as a treatment for atrioventricular (AV) block are increasing worldwide. Prevention strategies for AV block are lacking because modifiable risk factors have not yet been identified.
Objective: To identify risk factors for AV block in community-dwelling individuals.
Design, setting, and participants: In this population-based cohort study, data from the Mini-Finland Health Survey, conducted from January 1, 1978, to December 31, 1980, were used to examine demographics, comorbidities, habits, and laboratory and electrocardiographic (ECG) measurements as potential risk factors for incident AV block. Data were ascertained during follow-up from January 1, 1987, through December 31, 2011, using a nationwide registry. A total of 6146 community-dwelling individuals were included in the analysis performed from January 15 through April 3, 2018.
Main outcomes and measures: Incidence of AV block (hospitalization for second- or third-degree AV block).
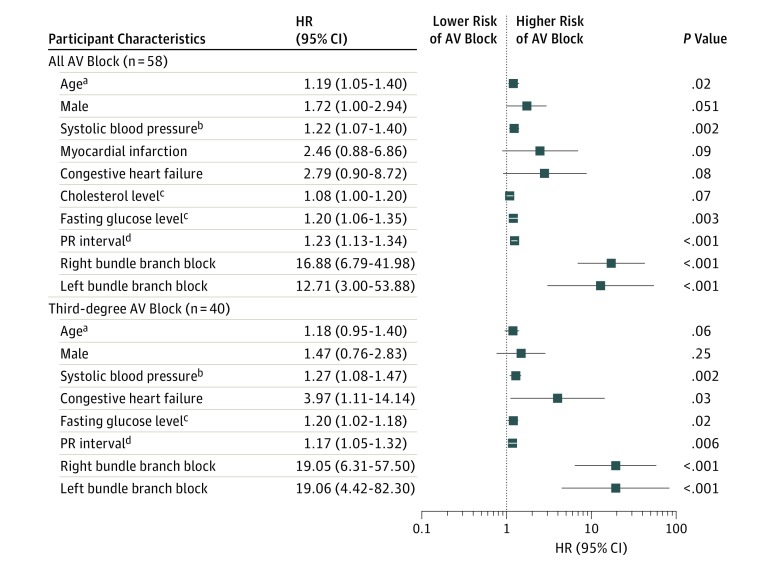
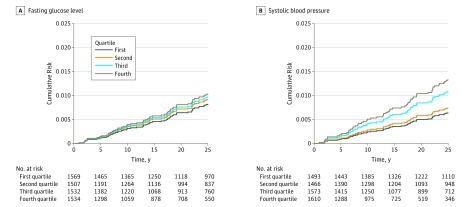
Results: Among the 6146 participants (3449 [56.1%] women; mean [SD] age, 49.2 [12.9] years), 529 (8.6%) had ECG evidence of conduction disease and 58 (0.9%) experienced a hospitalization with AV block. Older age (hazard ratio [HR] per 5-year increment, 1.34; 95% CI, 1.16-1.54; P < .001), male sex (HR, 2.04; 95% CI, 1.19-3.45; P = .01), a history of myocardial infarction (HR, 3.54; 95% CI, 1.33-9.42; P = .01), and a history of congestive heart failure (HR, 3.33; 95% CI, 1.10-10.09; P = .03) were each independently associated with AV block. Two modifiable risk factors were also independently associated with AV block. Every 10-mm Hg increase in systolic blood pressure was associated with a 22% higher risk (HR, 1.22; 95% CI, 1.10-1.34; P = .005), and every 20-mg/dL increase in fasting glucose level was associated with a 22% higher risk (HR, 1.22; 95% CI, 1.08-1.35; P = .001). Both risk factors remained statistically significant (HR for systolic blood pressure, 1.26 [95% CI, 1.06-1.49; P = .007]; HR for glucose level, 1.22 [95% CI, 1.04-1.43; P = .01]) after adjustment for major adverse coronary events during the follow-up period. In population-attributable risk assessment, an estimated 47% (95% CI, 8%-67%) of AV blocks may have been avoided if all participants exhibited ideal blood pressure and 11% (95% CI, 2%-21%) may have been avoided if all had a normal fasting glucose level.
Conclusions and relevance: In this analysis of data from a population-based cohort study, suboptimal blood pressure and fasting glucose level were associated with AV block. These results suggest that a large proportion of AV blocks are assocated with these risk factors, even after adjusting for other major adverse coronary events.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
