

Evaluation of RESPOND, a patient-centred program to prevent falls in older people presenting to the emergency department with a fall: A randomised controlled trial
- PMID: 31125354
- PMCID: PMC6534288
- DOI: 10.1371/journal.pmed.1002807
Evaluation of RESPOND, a patient-centred program to prevent falls in older people presenting to the emergency department with a fall: A randomised controlled trial
Abstract
Background: Falls are a leading reason for older people presenting to the emergency department (ED), and many experience further falls. Little evidence exists to guide secondary prevention in this population. This randomised controlled trial (RCT) investigated whether a 6-month telephone-based patient-centred program-RESPOND-had an effect on falls and fall injuries in older people presenting to the ED after a fall.
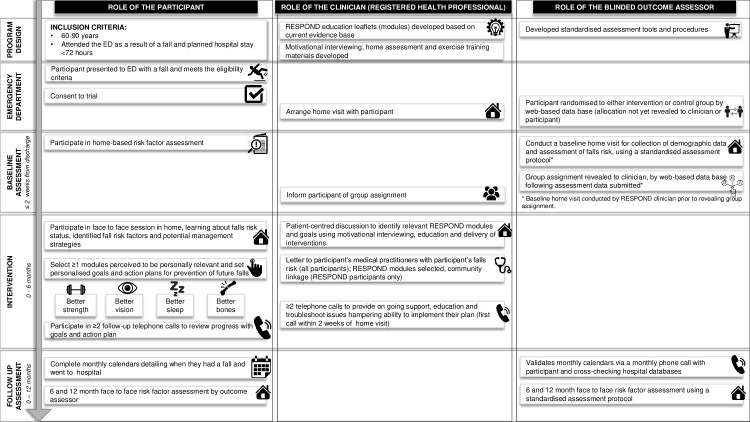
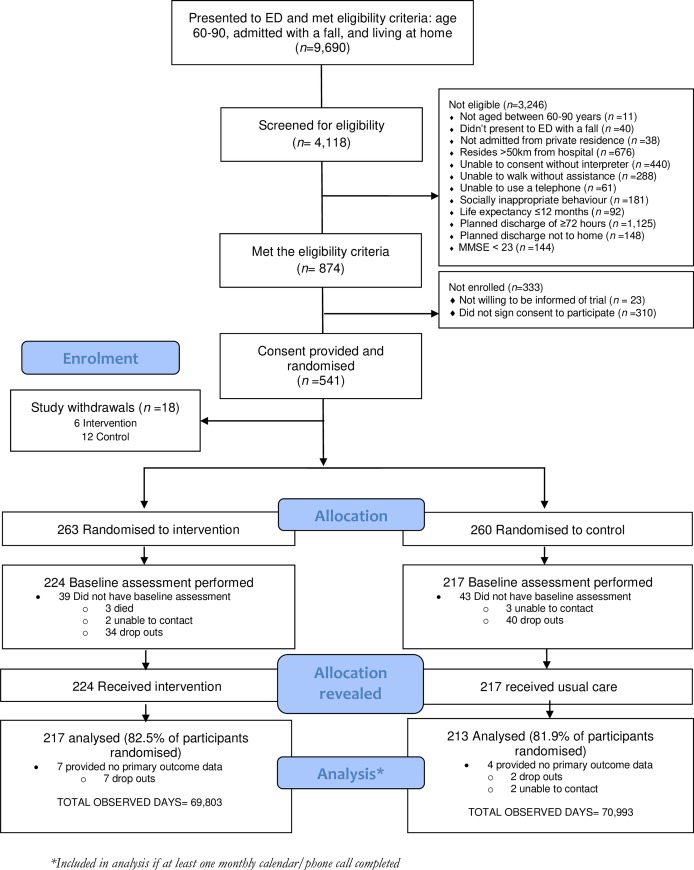
Methods and findings: Community-dwelling people aged 60-90 years presenting to the ED with a fall and planned for discharge home within 72 hours were recruited from two EDs in Australia. Participants were enrolled if they could walk without hands-on assistance, use a telephone, and were free of cognitive impairment (Mini-Mental State Examination > 23). Recruitment occurred between 1 April 2014 and 29 June 2015. Participants were randomised to receive either RESPOND (intervention) or usual care (control). RESPOND comprised (1) home-based risk assessment; (2) 6 months telephone-based education, coaching, goal setting, and support for evidence-based risk factor management; and (3) linkages to existing services. Primary outcomes were falls and fall injuries in the 12-month follow-up. Secondary outcomes included ED presentations, hospital admissions, fractures, death, falls risk, falls efficacy, and quality of life. Assessors blind to group allocation collected outcome data via postal calendars, telephone follow-up, and hospital records. There were 430 people in the primary outcome analysis-217 randomised to RESPOND and 213 to control. The mean age of participants was 73 years; 55% were female. Falls per person-year were 1.15 in the RESPOND group and 1.83 in the control (incidence rate ratio [IRR] 0.65 [95% CI 0.43-0.99]; P = 0.042). There was no significant difference in fall injuries (IRR 0.81 [0.51-1.29]; P = 0.374). The rate of fractures was significantly lower in the RESPOND group compared with the control (0.05 versus 0.12; IRR 0.37 [95% CI 0.15-0.91]; P = 0.03), but there were no significant differences in other secondary outcomes between groups: ED presentations, hospitalisations or falls risk, falls efficacy, and quality of life. There were two deaths in the RESPOND group and one in the control group. No adverse events or unintended harm were reported. Limitations of this study were the high number of dropouts (n = 93); possible underreporting of falls, fall injuries, and hospitalisations across both groups; and the relatively small number of fracture events.
Conclusions: In this study, providing a telephone-based, patient-centred falls prevention program reduced falls but not fall injuries, in older people presenting to the ED with a fall. Among secondary outcomes, only fractures reduced. Adopting patient-centred strategies into routine clinical practice for falls prevention could offer an opportunity to improve outcomes and reduce falls in patients attending the ED.
Trial registration: Australian New Zealand Clinical Trials Registry (ACTRN12614000336684).
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: TH reports personal fees from DorsaVi Pty, Ltd., for provision of economic evaluation consultancy service. DA and RM report salaries supported by the NHMRC for project funding as part of the Partnership Projects scheme. AB and JL report grants from the NHMRC during the conduct of the study. EB and EM report grants from the NHMRC supporting their salaries. All other authors have no conflicts of interest.
Figures
Similar articles
-
A mixed methods process evaluation of a person-centred falls prevention program.BMC Health Serv Res. 2019 Nov 28;19(1):906. doi: 10.1186/s12913-019-4614-z. BMC Health Serv Res. 2019. PMID: 31779624 Free PMC article. Clinical Trial.
-
RESPOND--A patient-centred programme to prevent secondary falls in older people presenting to the emergency department with a fall: protocol for a multicentre randomised controlled trial.Inj Prev. 2015 Feb;21(1):e1. doi: 10.1136/injuryprev-2014-041271. Epub 2014 Jun 23. Inj Prev. 2015. PMID: 24958769 Clinical Trial.
-
RESPOND: a patient-centred programme to prevent secondary falls in older people presenting to the emergency department with a fall-protocol for a mixed methods programme evaluation.Inj Prev. 2016 Apr;22(2):153-60. doi: 10.1136/injuryprev-2014-041453. Epub 2014 Nov 12. Inj Prev. 2016. PMID: 25392367
-
Multifactorial falls prevention programmes for older adults presenting to the emergency department with a fall: systematic review and meta-analysis.Inj Prev. 2019 Dec;25(6):557-564. doi: 10.1136/injuryprev-2019-043214. Epub 2019 Jul 9. Inj Prev. 2019. PMID: 31289112
-
Deprescribing fall-risk increasing drugs (FRIDs) for the prevention of falls and fall-related complications: a systematic review and meta-analysis.BMJ Open. 2021 Feb 10;11(2):e035978. doi: 10.1136/bmjopen-2019-035978. BMJ Open. 2021. PMID: 33568364 Free PMC article.
Cited by
-
Digital Health Coaching Programs Among Older Employees in Transition to Retirement: Systematic Literature Review.J Med Internet Res. 2020 Sep 24;22(9):e17809. doi: 10.2196/17809. J Med Internet Res. 2020. PMID: 32969827 Free PMC article. Review.
-
Psychological and educational interventions for preventing falls in older people living in the community.Cochrane Database Syst Rev. 2024 Oct 3;10(10):CD013480. doi: 10.1002/14651858.CD013480.pub2. Cochrane Database Syst Rev. 2024. PMID: 39360568
-
How Modifiable Are Modifiable Dementia Risk Factors? A Framework for Considering the Modifiability of Dementia Risk Factors.J Prev Alzheimers Dis. 2024;11(1):22-37. doi: 10.14283/jpad.2023.119. J Prev Alzheimers Dis. 2024. PMID: 38230714 Free PMC article. Review.
-
A mixed methods process evaluation of a person-centred falls prevention program.BMC Health Serv Res. 2019 Nov 28;19(1):906. doi: 10.1186/s12913-019-4614-z. BMC Health Serv Res. 2019. PMID: 31779624 Free PMC article. Clinical Trial.
-
Experiences of Patient-Centered Care Among Older Community-Dwelling Australians.Front Public Health. 2022 Jun 14;10:912137. doi: 10.3389/fpubh.2022.912137. eCollection 2022. Front Public Health. 2022. PMID: 35774564 Free PMC article.
References
-
- Institute of Medicine. Hospital-Based Emergency Care: At the Breaking Point. Washington, DC: The National Academies Press; 2007. 424 p.
-
- Burkett E, Martin-Khan MG, Scott J, Samanta M, Gray LC. Trends and predicted trends in presentations of older people to Australian emergency departments: effects of demand growth, population aging and climate change. Aust Health Rev. 2016;41(3):246–53. - PubMed
-
- Stathakis V, Gray S, Berecki-Gisolf J. Fall-related injury profile for Victorians aged 65 years and older Monash University Accident Research Centre (MUARC); 2015.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
