

Preoperative D-dimer and Gamma-Glutamyltranspeptidase Predict Major Complications and Survival in Colorectal Liver Metastases Patients After Resection
- PMID: 31125760
- PMCID: PMC6531870
- DOI: 10.1016/j.tranon.2019.04.011
Preoperative D-dimer and Gamma-Glutamyltranspeptidase Predict Major Complications and Survival in Colorectal Liver Metastases Patients After Resection
Abstract
Objectives: To investigate the predictive value of the pre-operative D-dimer and gamma-glutamyltranspeptidase (GGT) for the prognosis in colorectal liver metastases (CRLM) patients after hepatic resection.
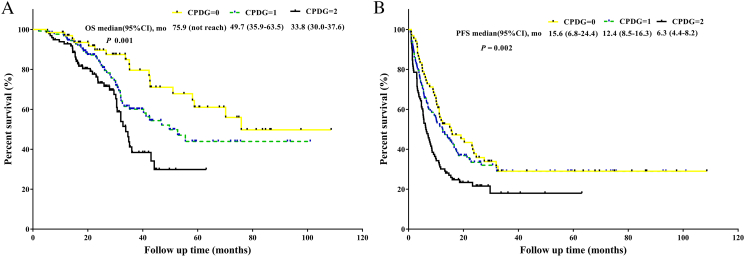
Methods: Two hundred and ninety-two patients between December 2008 and December 2016 and 101 patients at our center from January 2017 to December 2018 were selected as a training set and validation set, respectively. The combination of the pre-operative D-dimer and GGT status (CPDG score) was scored as follows: elevated D-dimer levels with elevated GGT levels was allocated a score of 2, decreased D-dimer levels with decreased GGT levels was allocated a score of 0, and all other combinations were allocated a score of 1. In the training set, a logistic regression was applied to explore potential predictors of major postoperative complications. A Cox proportional hazards analysis was used to analyze survival. We further verified our findings in the validation set.
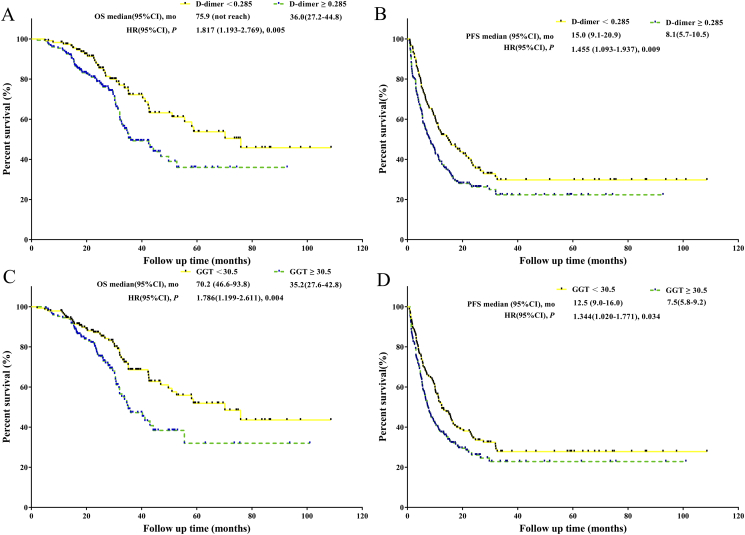
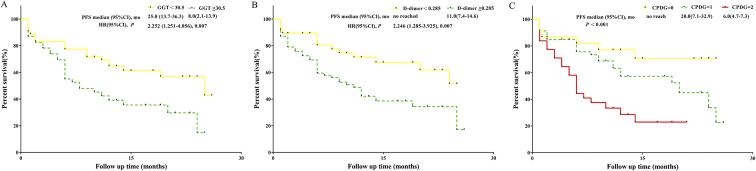
Results: Major complications occurred in 43 (14.7%) and 25 (24.8%) patients in the training set and validation set, respectively. In the training set, multivariate analysis showed that elevated GGT levels and elevated D-dimer levels independently predicted major complications respectively. In the multivariate analyses, elevated pre-operative D-dimer levels remained independently associated with decreased overall survival (OS) (hazard ratio [HR] = 1.751, 95% confidence interval [CI]: 1.139-2.691, P = .01). The CPDG score was an independent prognostic factor for major complications and OS in the multivariate analyses. The predictive ability of the CPDG score was higher than either factor alone. A Kaplan-Meier survival analysis showed that compared with patients with CPDG score = 1 or CPDG score = 0, patients with a CPDG score = 2 had worsened OS. Furthermore, for OS comparisons, the differences between any two groups were significant. In the validation set, elevated GGT and D-dimer were also suggested to predict worse progression-free survival (PFS) and to be independently associated with major complications.
Conclusions: The pre-operative D-dimer levels, GGT levels and CPDG score are reliable biomarkers to predict post-operative major complications or survival in CRLM patients after hepatic resection, which make it useful for CRLM patients in guiding surveillance approaches and prognosis assessments.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Van Cutsem E, Nordlinger B, Adam R, Kohne CH, Pozzo C, Poston G, Ychou M, Rougier P. Towards a pan-European consensus on the treatment of patients with colorectal liver metastases. Eur J Cancer. 2006;42(14):2212–2221. - PubMed
-
- Section of Gastrointestinal Surgery B CMASoCASB, Chinese Medical Association Guideline for the diagnosis and comprehensive treatment of colorectal cancer with liver metastases (2016 edition) Chin J Dig Surg. 2016;(15):755–767.
-
- Cucchetti A, Ferrero A, Cescon M, Donadon M, Russolillo N, Ercolani G, Stacchini G, Mazzotti F, Torzilli G, Pinna AD. Cure model survival analysis after hepatic resection for colorectal liver metastases. Ann Surg Oncol. 2015;22(6):1908–1914. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
